Anatomy and physiology account for a significant portion of the CST exam — embedded in nearly every question about surgical procedures, patient positioning, instrumentation, and pathology. This lesson condenses a full A&P curriculum into the structures, terms, and physiological concepts you must know for exam day and for every case you scrub.
1. Foundational Concepts & Anatomical Terminology
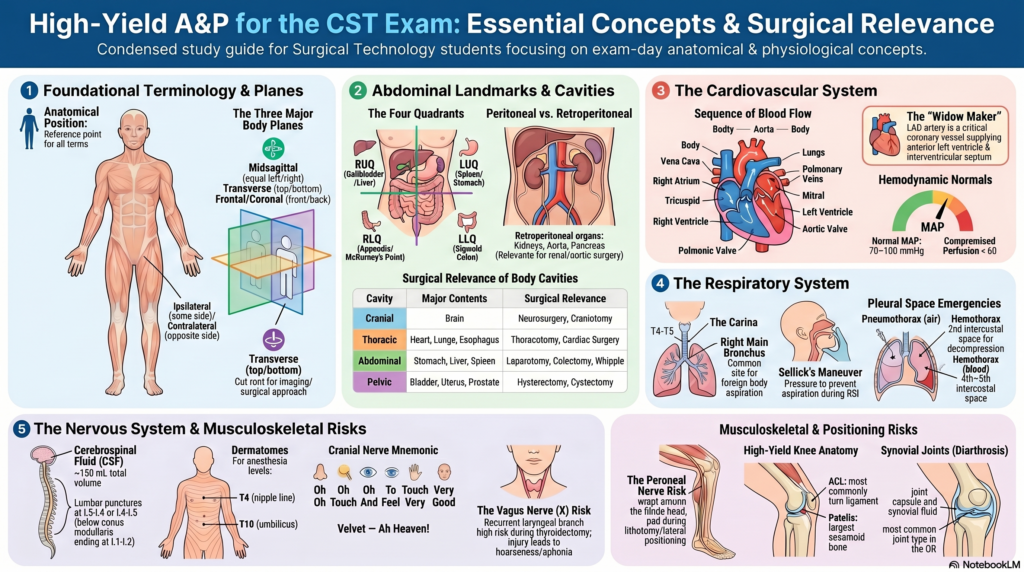
1A. Anatomical Position & Directional Terms
Anatomical position: Body erect, face forward, arms at sides with palms facing forward. All directional terms are based on this position, regardless of the patient’s actual positioning.
| Term | Meaning | Example |
|---|---|---|
| Superior / Cranial | Toward the head | The heart is superior to the liver |
| Inferior / Caudal | Toward the feet | The bladder is inferior to the uterus |
| Anterior / Ventral | Toward the front | The sternum is anterior to the heart |
| Posterior / Dorsal | Toward the back | The spine is posterior to the esophagus |
| Medial | Toward the midline | The nose is medial to the eyes |
| Lateral | Away from the midline | The ears are lateral to the nose |
| Proximal | Closer to the point of origin/attachment | The elbow is proximal to the wrist |
| Distal | Further from the point of origin/attachment | The fingers are distal to the elbow |
| Superficial | Toward the surface | Skin is superficial to muscle |
| Deep | Away from the surface | Bone is deep to muscle |
| Ipsilateral | Same side of the body | The right arm and right leg are ipsilateral |
| Contralateral | Opposite side of the body | The right arm and left leg are contralateral |
1B. Body Planes
Sagittal Plane
Divides the body into left and right; midsagittal = equal halves
Frontal (Coronal) Plane
Divides the body into anterior (front) and posterior (back)
Transverse (Horizontal) Plane
Divides the body into superior (top) and inferior (bottom)
Oblique Plane
Any diagonal cut across the body; commonly referenced in imaging
1C. Body Cavities
| Cavity | Contents | Surgical Relevance |
|---|---|---|
| Cranial | Brain | Neurosurgery; ICP monitoring; craniotomy |
| Spinal (Vertebral) | Spinal cord | Laminectomy, spinal fusion, discectomy |
| Thoracic | Heart, lungs, great vessels, esophagus, trachea; divided by the mediastinum | Cardiac surgery, thoracotomy, pneumonectomy, esophagectomy |
| Abdominal | Stomach, intestines, liver, spleen, pancreas, kidneys (retroperitoneal) | Laparotomy, appendectomy, colectomy, Whipple procedure |
| Pelvic | Urinary bladder, rectum, uterus/ovaries/prostate | Hysterectomy, prostatectomy, cystectomy, rectal resection |
| Peritoneal vs. Retroperitoneal | Peritoneal: covered by peritoneum (stomach, liver, spleen); Retroperitoneal: behind peritoneum (kidneys, aorta, IVC, pancreas, duodenum) | Retroperitoneal approach: renal, aortic, adrenal surgery |
1D. Abdominal Quadrants & Regions
The abdomen is divided into four quadrants (RUQ, LUQ, RLQ, LLQ) for clinical use and nine regions for anatomical description.
| Quadrant | Major Organs | Surgical Significance |
|---|---|---|
| RUQ (Right Upper) | Liver, gallbladder, right kidney, hepatic flexure of colon, duodenum, head of pancreas | Cholecystectomy, hepatic resection, Whipple |
| LUQ (Left Upper) | Spleen, stomach, left kidney, splenic flexure of colon, body/tail of pancreas | Splenectomy, distal pancreatectomy, gastric surgery |
| RLQ (Right Lower) | Appendix, cecum, terminal ileum, right ureter, right ovary/tube, ascending colon | Appendectomy; McBurney’s point (1/3 from ASIS to umbilicus) |
| LLQ (Left Lower) | Sigmoid colon, descending colon, left ureter, left ovary/tube | Sigmoid colectomy, diverticulitis surgery |
1E. Tissue Types
| Tissue Type | Function | Examples / OR Relevance |
|---|---|---|
| Epithelial | Lines/covers surfaces; protection, secretion, absorption | Skin, GI tract lining, glands; wound healing requires epithelialization |
| Connective | Supports, connects, binds structures | Bone, cartilage, tendons, ligaments, fascia, adipose, blood |
| Muscle | Movement, pumping, peristalsis | Skeletal (voluntary), cardiac (involuntary striated), smooth (involuntary non-striated) |
| Nervous | Electrical signal transmission; control and coordination | Neurons, neuroglia; brain, spinal cord, peripheral nerves |
2. Cardiovascular System
2A. The Heart
The heart is a four-chambered muscular pump located in the mediastinum, slightly left of the midline, surrounded by the pericardium (fibrous outer + serous inner layers).
- Right atrium → receives deoxygenated blood from superior/inferior vena cava (SVC/IVC) and coronary sinus
- Right ventricle → pumps blood through pulmonic valve → pulmonary artery → lungs (pulmonary circulation)
- Left atrium → receives oxygenated blood from four pulmonary veins
- Left ventricle → thickest wall; pumps through aortic valve → aorta → systemic circulation
- Tricuspid valve (right AV): between right atrium and right ventricle (3 leaflets)
- Mitral (bicuspid) valve (left AV): between left atrium and left ventricle (2 leaflets)
- Papillary muscles + chordae tendineae — prevent AV valve prolapse during systole
Blood Flow Through the Heart (in order):
Body → SVC/IVC → Right Atrium → Tricuspid valve → Right Ventricle → Pulmonic valve → Pulmonary artery → Lungs → Pulmonary veins → Left Atrium → Mitral valve → Left Ventricle → Aortic valve → Aorta → Body
2B. Cardiac Conduction System
- SA node (sinoatrial) — natural pacemaker; in right atrium; generates impulse 60–100 bpm
- AV node (atrioventricular) — delays impulse allowing ventricles to fill; located at junction of atria and ventricles
- Bundle of His → Right & Left Bundle Branches → Purkinje fibers → ventricular myocardium contraction
- EKG waves: P wave = atrial depolarization; QRS complex = ventricular depolarization; T wave = ventricular repolarization
- Systole = contraction (ventricles pump); Diastole = relaxation (ventricles fill)
2C. Coronary Arteries
- Right Coronary Artery (RCA) — supplies right ventricle, inferior left ventricle, SA and AV nodes (in most people)
- Left Main Coronary Artery → divides into:
- Left Anterior Descending (LAD) — “widow maker”; supplies anterior left ventricle, interventricular septum
- Left Circumflex (LCx) — supplies lateral left ventricle, left atrium
- Coronary arteries fill during diastole (not systole)
2D. Major Blood Vessels
| Vessel | Type | Location / Surgical Relevance |
|---|---|---|
| Aorta | Artery | Largest artery; ascending → arch → descending thoracic → abdominal → bifurcates at L4 into common iliac arteries; AAA repair |
| Superior Vena Cava (SVC) | Vein | Returns blood from upper body to right atrium; CVP lines placed here |
| Inferior Vena Cava (IVC) | Vein | Returns blood from lower body; IVC filter placement; compression during prone positioning |
| Femoral Artery | Artery | Femoral triangle; arterial access for cardiac cath, bypass cannulation, endovascular procedures |
| Carotid Arteries | Artery | Common carotid → internal (brain) + external (face); carotid endarterectomy (CEA) |
| Portal Vein | Vein | Drains GI tract to liver; portal hypertension in liver disease |
| Saphenous Vein | Vein | Longest vein in body; harvested for CABG graft; varicose veins |
2E. Blood Pressure & Hemodynamic Concepts
- Blood pressure = Cardiac Output (CO) × Systemic Vascular Resistance (SVR)
- Cardiac Output (CO) = Heart Rate (HR) × Stroke Volume (SV); normal ~5 L/min
- Mean Arterial Pressure (MAP) = Diastolic + 1/3(Systolic − Diastolic); normal 70–100 mmHg; minimum 60 mmHg to perfuse organs
- Normal BP: 120/80 mmHg; Hypotension in OR: systolic <90 or MAP <60
- Preload: volume returning to heart (venous return); Afterload: resistance the heart pumps against; Contractility: intrinsic pumping force
3. Respiratory System
3A. Upper Airway Structures
- Nasal cavity — warms, humidifies, and filters air; nasal turbinates increase surface area
- Pharynx — nasopharynx (posterior to nasal cavity), oropharynx (posterior to oral cavity), laryngopharynx (hypopharynx)
- Epiglottis — leaf-shaped cartilage; covers larynx during swallowing; critical anatomical landmark for intubation
- Larynx — voice box; contains vocal cords (true and false); protected anteriorly by thyroid cartilage (“Adam’s apple”); cricothyroid membrane — emergency airway access site (cricothyrotomy)
- Glottis — opening between vocal cords; narrowest point of adult airway; target for ETT placement
- Cricoid cartilage — only complete ring of tracheal cartilage; site of Sellick’s maneuver (cricoid pressure) during RSI
3B. Lower Airway Structures
- Trachea — 10–15 cm long; 16–20 C-shaped cartilaginous rings; bifurcates at carina (T4–T5 level) into right and left main bronchi
- Right main bronchus — shorter, wider, more vertical than left → most common site for foreign body aspiration and inadvertent endobronchial intubation
- Bronchi → lobar bronchi (3 right, 2 left) → segmental bronchi → bronchioles → terminal bronchioles → respiratory bronchioles → alveolar ducts → alveoli
- Alveoli — site of gas exchange (O₂/CO₂); lined with Type I pneumocytes (gas exchange) and Type II pneumocytes (produce surfactant); ~300 million alveoli; surrounded by pulmonary capillaries
- Surfactant — reduces alveolar surface tension; prevents alveolar collapse (atelectasis); deficient in premature infants (RDS — Respiratory Distress Syndrome)
3C. Lungs & Pleura
- Right lung — 3 lobes (upper, middle, lower); 10 segments; larger than left
- Left lung — 2 lobes (upper, lower); 8–9 segments; has cardiac notch and lingula (corresponds to right middle lobe)
- Pleura — visceral pleura (covers lung) + parietal pleura (lines thoracic wall); pleural space between them is a potential space containing <15 mL serous fluid
- Pneumothorax — air in pleural space; lung collapses; tension pneumothorax = medical emergency (needle decompression at 2nd ICS, MCL)
- Hemothorax — blood in pleural space; chest tube insertion at 4th–5th ICS, MAL
- Hilum — root of lung; where bronchi, pulmonary vessels, lymphatics, and nerves enter/exit
3D. Respiratory Physiology
- Inspiration (active): diaphragm contracts (moves down), external intercostals contract → thoracic volume increases → pressure decreases → air flows in
- Expiration (passive at rest): diaphragm relaxes → thoracic volume decreases → air flows out
- Tidal Volume (TV) — volume per normal breath ~500 mL; Minute Volume = TV × RR (~7,500 mL/min)
- SpO₂ — pulse oximetry; normal >95%; <90% = hypoxia requiring intervention
- EtCO₂ (end-tidal CO₂) — exhaled CO₂ measurement; normal 35–45 mmHg; confirms ETT placement; earliest sign of MH
- PaO₂ — arterial O₂ tension; normal 80–100 mmHg; PaCO₂ — arterial CO₂; normal 35–45 mmHg
- Diaphragm — primary muscle of respiration; innervated by phrenic nerve (C3-4-5)
4. Nervous System
4A. Organization of the Nervous System
Central Nervous System (CNS)
Brain + Spinal cord; enclosed by bone and meninges; protected by blood-brain barrier (BBB)
Peripheral Nervous System (PNS)
All nervous tissue outside CNS; 12 cranial nerves + 31 spinal nerve pairs + autonomic nerves
4B. The Brain
| Structure | Function | Surgical Relevance |
|---|---|---|
| Frontal lobe | Motor cortex, personality, executive function, speech (Broca’s area — left side) | Frontal craniotomy; tumors here cause personality change, motor deficits |
| Parietal lobe | Sensory processing, spatial awareness | Lesions cause contralateral sensory deficits |
| Temporal lobe | Hearing, memory, language comprehension (Wernicke’s area) | Temporal lobe epilepsy; acoustic neuroma |
| Occipital lobe | Visual processing | Visual field deficits from lesions |
| Cerebellum | Coordination, balance, fine motor control | Posterior fossa craniotomy; seated/park bench position |
| Brainstem | Vital functions: breathing, HR, blood pressure, consciousness; connects brain to spinal cord | Brainstem lesions → life-threatening; extreme caution during surgery near foramen magnum |
| Hypothalamus | Temperature regulation, appetite, hormone control, circadian rhythm | Thermoregulation disrupted under anesthesia; hypothermia risk |
4C. Meninges & Cerebrospinal Fluid (CSF)
- Dura mater — outermost; tough fibrous; epidural space is between dura and vertebral bone
- Arachnoid mater — middle; subarachnoid space below contains CSF
- Pia mater — innermost; adheres directly to brain/cord surface
- CSF — clear fluid; produced by choroid plexus in ventricles; cushions brain/cord; total volume ~150 mL; circulates through ventricles → subarachnoid space → absorbed at arachnoid granulations
- Lumbar puncture (LP) — spinal tap; performed at L3-L4 or L4-L5 (below conus medullaris at L1-L2); spinal anesthesia injected here
- Intracranial Pressure (ICP) — normal 5–15 mmHg; elevated ICP >20 mmHg = emergency; signs: Cushing’s triad (hypertension + bradycardia + irregular respirations)
4D. Spinal Cord & Nerve Roots
- Extends from brainstem to conus medullaris at L1–L2; below = cauda equina (“horse’s tail”) — floating nerve roots
- 31 pairs of spinal nerves: 8 cervical (C1–C8), 12 thoracic (T1–T12), 5 lumbar (L1–L5), 5 sacral (S1–S5), 1 coccygeal
- Dermatomes — skin areas innervated by specific spinal nerves; key landmarks: T4 = nipple line; T10 = umbilicus; L4 = knee; used to check level of spinal anesthesia
- Important plexuses: Brachial plexus (C5–T1) — upper extremity; Lumbar plexus (L1–L4) — anterior thigh/groin; Sacral plexus (L4–S3) — posterior thigh/leg (sciatic nerve)
4E. Autonomic Nervous System
| Division | Neurotransmitter | Effect | OR Example |
|---|---|---|---|
| Sympathetic (“fight or flight”) | Norepinephrine (NE) / Epinephrine | ↑HR, ↑BP, bronchodilation, pupil dilation, ↓GI motility, vasoconstriction | Epinephrine used for anaphylaxis/cardiac arrest; phenylephrine for hypotension |
| Parasympathetic (“rest and digest”) | Acetylcholine (ACh) | ↓HR, ↑GI motility, pupil constriction, bronchoconstriction, increased secretions | Atropine/glycopyrrolate block parasympathetic effects (bradycardia, secretions); neostigmine enhances ACh |
4F. Cranial Nerves — The 12 Pairs
| # | Name | Function | Surgical Relevance |
|---|---|---|---|
| I | Olfactory | Smell | Anterior cranial fossa; esthesioneuroblastoma |
| II | Optic | Vision | Protect during orbital/skull base surgery; assess postop visual acuity |
| III | Oculomotor | Eye movement (most), pupil constriction, eyelid elevation | Fixed dilated pupil = CN III compression = herniation warning |
| IV | Trochlear | Superior oblique eye movement | Orbital surgery |
| V | Trigeminal | Facial sensation (3 branches: ophthalmic V1, maxillary V2, mandibular V3); mastication (V3) | Trigeminal neuralgia; dental/maxillofacial surgery; local anesthetic nerve blocks |
| VI | Abducens | Lateral eye movement | Strabismus surgery |
| VII | Facial | Facial expression, taste (anterior 2/3 tongue), lacrimation, salivation | At risk during parotid, mastoid, acoustic neuroma surgery; facial nerve monitoring |
| VIII | Vestibulocochlear | Hearing and balance | Acoustic neuroma resection; cochlear implant surgery |
| IX | Glossopharyngeal | Taste (posterior 1/3 tongue), swallowing, carotid body/sinus | Tonsillectomy; carotid surgery risk |
| X | Vagus | Parasympathetic to thorax/abdomen; voice (recurrent laryngeal branch); heart rate | Recurrent laryngeal nerve at risk in thyroidectomy, carotid, esophageal surgery → hoarseness/aphonia if injured |
| XI | Accessory (Spinal) | Trapezius and sternocleidomastoid muscle movement | At risk during posterior triangle neck dissection |
| XII | Hypoglossal | Tongue movement | At risk during carotid endarterectomy; injury causes tongue deviation |
Memory Aid for cranial nerves: “Oh Oh Oh To Touch And Feel Very Good Velvet — Ah Heaven!” (Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal)
5. Musculoskeletal System
5A. Bone Structure & Classification
- Periosteum — outer fibrous membrane; contains blood vessels and osteoblasts; stripped during fracture repair
- Cortical (compact) bone — dense outer layer; greatest strength
- Cancellous (spongy/trabecular) bone — inner lattice network; contains red marrow (blood cell production)
- Endosteum — lines medullary canal (yellow marrow in adults)
- Long bones (femur, humerus) — epiphysis (ends) + diaphysis (shaft) + metaphysis (growth plate region)
- Osteoblasts — build bone; Osteoclasts — resorb bone; Osteocytes — mature bone cells maintaining matrix
5B. Key Bones — Surgical Landmarks
| Bone / Landmark | Location | Surgical Relevance |
|---|---|---|
| Sternum | Anterior chest wall; manubrium + body + xiphoid process | Median sternotomy for cardiac surgery; Angle of Louis (sternal angle) = T4 level |
| Clavicle | Between sternum and acromion | Subclavian vein landmark; brachial plexus block reference; ORIF for fractures |
| Iliac Crest (ASIS) | Anterosuperior iliac spine; pelvic brim | Bone graft donor site; McBurney’s point landmark; anterior approach hip; positioning landmark |
| Greater Trochanter | Lateral prominence of proximal femur | Hip arthroplasty; lateral approach to hip; padding required in lateral positioning |
| Tibial Tuberosity | Anterior proximal tibia; patellar tendon insertion | IO access site in pediatric emergencies; Osgood-Schlatter disease |
| Fibula Head | Lateral aspect of knee | Peroneal nerve wraps around here → at risk with lateral leg position; must pad in lithotomy |
| Medial Epicondyle of Humerus | Medial elbow | Ulnar nerve (“funny bone”) at risk with elbow pressure; must pad in lateral and prone positioning |
5C. Joints
| Joint Type | Characteristics | Examples / OR Relevance |
|---|---|---|
| Synarthrosis (fibrous) | Immovable; united by fibrous tissue | Skull sutures; teeth in sockets |
| Amphiarthrosis (cartilaginous) | Slightly movable; united by cartilage | Intervertebral discs, pubic symphysis |
| Diarthrosis (synovial) | Freely movable; synovial fluid in joint capsule; most common joint type | Knee, hip, shoulder, elbow — arthroscopy, arthroplasty; lined by synovial membrane; articular cartilage covers bone ends |
5D. Knee Anatomy (High-Yield for CST)
- ACL (Anterior Cruciate Ligament) — prevents anterior tibial displacement; most commonly torn ligament; ACL reconstruction (arthroscopic)
- PCL (Posterior Cruciate Ligament) — prevents posterior tibial displacement
- MCL (Medial Collateral Ligament) — medial stability
- LCL (Lateral Collateral Ligament) — lateral stability
- Medial and Lateral Menisci — fibrocartilage shock absorbers; meniscectomy or repair common
- Patella — largest sesamoid bone; articulates with femoral groove; patellar tendon connects to tibial tuberosity
5E. Muscle Physiology
- Sliding filament theory — actin (thin) and myosin (thick) filaments slide past each other during contraction; requires Ca²⁺ and ATP
- Motor unit — one motor neuron + all muscle fibers it innervates; neuromuscular junction (NMJ) = synapse between motor neuron and muscle
- Neuromuscular Junction — ACh released by motor neuron → binds nicotinic receptors on muscle → depolarization → contraction; NMBAs block this step
- Origin = stationary attachment; Insertion = movable attachment; muscle shortens from insertion toward origin
- Important muscles in positioning: Diaphragm (respiration), sternocleidomastoid (neck flexion/rotation), trapezius (shoulder elevation), gluteus maximus (hip extension), quadriceps (knee extension)