6. Gastrointestinal System
6A. GI Tract — Structure & Function
| Structure | Function | Surgical Relevance |
|---|---|---|
| Esophagus | Propels food from pharynx to stomach; ~25 cm; passes through diaphragm at esophageal hiatus (T10) | Esophagectomy; hiatal hernia repair (Nissen fundoplication); esophagoscopy; GERD |
| Stomach | Storage and initial digestion; produces HCl, pepsin, intrinsic factor; regions: cardia, fundus, body, pylorus. | Gastrectomy (partial/total); bariatric surgery (sleeve, bypass); peptic ulcer; gastrostomy |
| Small Intestine | Primary site of digestion and absorption; ~6–7 m; three segments: duodenum (25 cm), jejunum, ileum | Small bowel resection; Crohn’s disease; ileostomy; Meckel’s diverticulum |
| Large Intestine (Colon) | Water/electrolyte absorption; fecal formation; ~1.5 m; cecum → ascending → transverse → descending → sigmoid → rectum → anus | Colectomy; colostomy; hemorrhoidectomy; colonoscopy; colorectal cancer resection |
| Appendix | Vestigial; attached to cecum; lymphoid tissue | Appendectomy (most common emergent abdominal surgery); McBurney’s point |
| Rectum / Anus | Fecal storage and defecation; internal sphincter (involuntary) + external sphincter (voluntary) | Anterior resection; abdominoperineal resection (APR); hemorrhoidectomy; lithotomy position |
6B. Accessory Digestive Organs
| Organ | Function | Surgical Relevance |
|---|---|---|
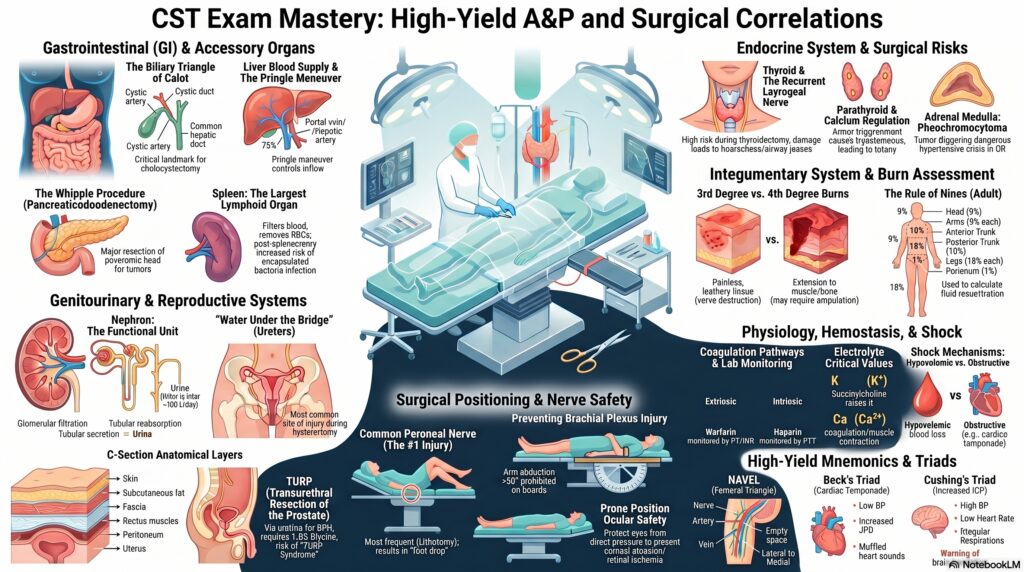
| Liver | Bile production; detoxification; protein synthesis (albumin, clotting factors); glycogen storage; drug metabolism; largest internal organ (1,200–1,500 g); 2 lobes (right is larger); receives dual blood supply (portal vein 75% + hepatic artery 25%) | Hepatectomy (Pringle maneuver to control inflow); liver transplant; TIPS procedure; cirrhosis complications |
| Gallbladder | Stores and concentrates bile (produced by liver); contracts when CCK released after fatty meal → bile flows into duodenum via common bile duct | Cholecystectomy (laparoscopic vs. open); choledochoscopy; cholelithiasis; Calot’s triangle (cystic artery, cystic duct, common hepatic duct) |
| Pancreas | Exocrine: digestive enzymes (amylase, lipase, trypsinogen) into duodenum via pancreatic duct; Endocrine: insulin (beta cells) and glucagon (alpha cells) from islets of Langerhans | Whipple procedure (pancreaticoduodenectomy) for head of pancreas tumors; distal pancreatectomy; pancreatitis; ERCP |
| Spleen | Largest lymphoid organ; filters blood; removes old RBCs; immune function; located LUQ behind 9th–11th ribs; highly vascular (fragile) | Splenectomy; highest risk of injury in abdominal trauma; post-splenectomy → increased infection risk (especially encapsulated bacteria: Strep pneumoniae, H. flu, N. meningitidis) → vaccinate |
7. Genitourinary System
7A. Urinary System
- Kidneys — paired retroperitoneal organs at T12–L3; right kidney slightly lower (displaced by liver); receive 20–25% of cardiac output; functional unit = nephron (glomerulus + tubules)
- Nephron function — glomerular filtration → tubular reabsorption → tubular secretion → urine formation; kidneys filter ~180 L/day; produce ~1–2 L urine/day; normal urine output ≥0.5 mL/kg/hr
- Renal hilum — where renal artery, renal vein, ureter, lymphatics enter/exit; left renal vein longer (crosses aorta) — used in live donor nephrectomy
- Ureters — ~28 cm; carry urine from renal pelvis → bladder; three natural narrowings (UPJ, pelvic brim, UVJ) — sites for stone impaction; at risk during hysterectomy (“water under the bridge”)
- Urinary Bladder — pelvic organ; detrusor muscle; trigone = fixed triangle (two ureteral orifices + internal urethral orifice); cystoscopy port of entry
- Urethra — male ~20 cm (longer, higher risk of catheter trauma); female ~4 cm (shorter, higher UTI risk); prostatic urethra passes through prostate gland
| Procedure | Anatomy Involved | Key Notes |
|---|---|---|
| Nephrectomy (open/laparoscopic) | Kidney, renal vessels, adrenal gland, ureter | Lateral flank or supine; flank position requires kidney rest elevation |
| Cystoscopy / TURBT | Bladder via urethra | Lithotomy position; glycine or sterile water irrigation |
| TURP | Prostate via urethra | Glycine 1.5% irrigation; TURP syndrome risk; lithotomy position |
| Ureteroscopy / Lithotripsy | Ureter, renal pelvis | Kidney stones; laser lithotripsy (holmium laser); stone basket retrieval |
7B. Female Reproductive System
- Ovaries — produce ova and sex hormones (estrogen, progesterone); held by broad ligament and ovarian ligament
- Fallopian tubes — transport ova from ovary to uterus; site of fertilization; fimbriae sweep ova in; ectopic pregnancy most common here (ampulla)
- Uterus — fundus (top), body, cervix (bottom); endometrium (inner lining — shed during menstruation), myometrium (muscular middle), perimetrium (serosal outer)
- Cervix — connects uterus to vagina; os (opening); cervical cancer — Pap smear; LEEP procedure
- Broad ligament — double fold of peritoneum supporting uterus, tubes, ovaries; contains uterine vessels
- Key GYN procedures: TAH-BSO (total abdominal hysterectomy + bilateral salpingo-oophorectomy); laparoscopic hysterectomy; D&C; myomectomy; ovarian cystectomy; tubal ligation; cesarean section
7C. Male Reproductive System
- Testes — produce sperm (spermatogenesis) and testosterone; located in scrotum (cooler temp required for sperm); covered by tunica albuginea; seminoma = most common testicular tumor
- Epididymis — comma-shaped; site of sperm maturation and storage; posterior to testis; epididymitis = infection
- Vas deferens (ductus deferens) — carries sperm from epididymis to ejaculatory duct; vasectomy performed here
- Seminal vesicles, prostate, bulbourethral glands — accessory glands contributing to semen; prostate surrounds prostatic urethra; BPH causes urinary obstruction → TURP
- Key urologic procedures: Radical prostatectomy; orchiectomy; vasectomy; orchiopexy (undescended testis — cryptorchidism); hydrocelectomy; circumcision
8. Endocrine System
| Gland | Location | Key Hormones | Surgical Relevance |
|---|---|---|---|
| Pituitary | Sella turcica (sphenoid bone); “master gland” | GH, TSH, ACTH, FSH, LH, ADH (posterior), oxytocin | Transsphenoidal hypophysectomy (pituitary adenoma); Cushing’s disease |
| Thyroid | Anterior neck; 2 lobes + isthmus; butterfly-shaped | T3, T4 (metabolism), Calcitonin (↓Ca²⁺) | Thyroidectomy (total/partial); recurrent laryngeal nerve at risk; parathyroids at risk; thyroid storm perioperatively; hyperthyroidism prep with beta-blockers + iodine |
| Parathyroid | 4 glands on posterior thyroid | PTH → ↑Ca²⁺ (↑bone resorption, ↑renal reabsorption, ↑GI absorption) | Parathyroidectomy (hyperparathyroidism); inadvertent removal → hypocalcemia → tetany; intraoperative PTH assay used |
| Adrenal Glands | Atop each kidney; cortex + medulla | Cortex: cortisol (stress), aldosterone (Na/K), androgens; Medulla: epinephrine, norepinephrine | Adrenalectomy; pheochromocytoma (medulla tumor → hypertensive crisis); Cushing’s syndrome (excess cortisol); Conn’s syndrome (excess aldosterone) |
| Pancreas (Endocrine) | Islets of Langerhans: alpha (glucagon) and beta (insulin) cells | Insulin ↓blood glucose; Glucagon ↑blood glucose | Diabetic patients require perioperative glucose monitoring; insulinoma (hypoglycemia); perioperative glucose target <200 mg/dL |
| Gonads | Testes / Ovaries | Testosterone, estrogen, progesterone | Orchiectomy (testicular cancer, prostate cancer); oophorectomy (ovarian cancer, endometriosis) |
9. Integumentary System (Skin)
9A. Skin Layers
- Epidermis — outermost; avascular; 5 layers (from deep to superficial: stratum basale, spinosum, granulosum, lucidum, corneum); no pain receptors; barrier to infection; keratinocytes predominate; melanocytes produce melanin (deeper = less UV penetration)
- Dermis — vascularized; collagen (strength) and elastin (flexibility) from fibroblasts; contains hair follicles, sweat glands, sebaceous glands, sensory receptors (Meissner’s, Pacinian corpuscles); papillary dermis (superficial) and reticular dermis (deep)
- Hypodermis (subcutaneous) — not true skin layer; adipose tissue; insulation; shock absorption; site of SQ injections
9B. Burn Classification
| Degree | Depth | Appearance | Pain | Healing |
|---|---|---|---|---|
| 1st Degree (Superficial) | Epidermis only | Red, dry, no blisters | Painful | 3–5 days; no scarring |
| 2nd Degree (Partial Thickness) | Epidermis + superficial/deep dermis | Blisters; moist; red; blanches | Very painful | 2–3 weeks (superficial); skin grafting for deep |
| 3rd Degree (Full Thickness) | All skin layers; may include subcutaneous | White/brown/black; leathery; dry; no blisters | Painless (nerve destruction) | Requires skin grafting; significant scarring |
| 4th Degree | Full thickness + muscle/bone/tendon | Charred; eschar | Painless | May require amputation |
Rule of Nines (adult burn % TBSA): Head/neck = 9%; each arm = 9%; anterior trunk = 18%; posterior trunk = 18%; each leg = 18%; perineum = 1%. Used to calculate fluid resuscitation (Parkland formula: 4 mL/kg/% TBSA burned — half in first 8 hrs, half in next 16 hrs).
10. Lymphatic & Immune System
- Lymphatic vessels — collect interstitial fluid (lymph), returns it to circulation via thoracic duct (left side) and right lymphatic duct (right upper body) → subclavian veins
- Thoracic duct — largest lymphatic vessel; drains most of body (left side + both legs + abdomen) → left subclavian vein junction; injury during esophagectomy or neck surgery → chylothorax
- Lymph nodes — filter lymph; produce lymphocytes; regional nodes are sampled in oncologic surgery to determine metastasis (sentinel node biopsy)
- Sentinel lymph node — first node(s) receiving drainage from primary tumor; identified with isosulfan blue dye and/or technetium-99m radiotracer; biopsy determines whether cancer has spread (staging)
- Key lymph node groups (surgical): Axillary (breast/upper extremity drainage; sampled in mastectomy); cervical (head/neck cancers); inguinal (lower extremity/perineal drainage); para-aortic (abdominal/pelvic cancers)
- Spleen — largest lymphoid organ; filters blood; removes senescent RBCs; immune surveillance; splenectomy → increased risk of overwhelming post-splenectomy infection (OPSI) with encapsulated organisms
- Thymus — located in anterior mediastinum; T-lymphocyte maturation; atrophies after puberty; thymoma may cause myasthenia gravis → thymectomy
11. Obstetric & Breast Anatomy
11A. Cesarean Section Anatomy (C-Section)
The most commonly performed major surgery in the world. Layers incised (from superficial to deep):
- Skin (Pfannenstiel or vertical midline incision)
- Subcutaneous fat (Camper’s fascia)
- Fascia of Scarpa
- Fascia of the rectus abdominis (anterior rectus sheath)
- Rectus abdominis muscles (separated, not cut in Pfannenstiel)
- Peritoneum (visceral and parietal)
- Uterus (low transverse incision — lower uterine segment)
11B. Breast Anatomy
- Overlies pectoralis major muscle (2nd–6th ribs); suspensory ligaments of Cooper attach to skin and pectoralis fascia
- Quadrants: UOQ (upper outer), UIQ, LOQ, LIQ; axillary tail of Spence extends into axilla; most breast cancers occur in UOQ (50%)
- Lymph drainage: Primarily to axillary nodes (Level I–III); also internal mammary nodes; sentinel node biopsy standard for staging
- Key procedures: Lumpectomy (breast-conserving); mastectomy (simple/modified radical/radical); sentinel node biopsy; axillary node dissection; breast reconstruction (TRAM, DIEP, tissue expanders, implants)
12. Surgical Positioning — Anatomical Risks & Nerve Injuries
Understanding anatomy is critical to preventing positioning injuries. The CST exam frequently tests which nerves and structures are at risk in each position.
| Position | Anatomy / Nerves at Risk | Padding / Prevention | Common Procedures |
|---|---|---|---|
| Supine | Brachial plexus (arm abducted >90°); ulnar nerve (elbow); heel pressure (skin/achilles); occiput pressure | Arms ≤90° abduction; padded arm boards; pillow under knees; heel protectors | Abdominal, cardiac, vascular, GYN, orthopedic |
| Trendelenburg | Brachial plexus (shoulder braces push on nerve); increased ICP; airway edema; aspiration risk | Avoid shoulder braces; use non-slip mattress; head elevated slightly; limit duration | GYN laparoscopy, lower abdominal surgery, central line placement |
| Reverse Trendelenburg | Venous pooling in legs → hypotension; sliding off table | Padded footboard; sequential compression devices (SCDs) | Head/neck, thyroid, upper GI laparoscopy |
| Lithotomy | Common peroneal nerve at fibular head (most common positioning injury); femoral nerve; obturator nerve; lower extremity compartment syndrome; lumbar strain | Pad lateral knee/leg supports; lower both legs simultaneously; limit duration (<2 hrs if possible); avoid hip hyperflexion | GYN (perineal), urologic, rectal, obstetric |
| Prone | Eyes (corneal abrasion, retinal ischemia from direct pressure — MUST protect); brachial plexus; ulnar nerve (elbow); femoral nerve; breast/genitalia pressure; IVC compression → hypotension | Foam face rest or pins (Mayfield) for head; chest rolls/Wilson frame; arms in Superman or at side; protected eyes checked frequently; padded elbows and knees | Spinal/posterior neurosurgery, posterior orthopedic, posterior urologic |
| Lateral (Decubitus) | Brachial plexus (down-side axillary compression); common peroneal nerve (down-side fibular head); ear; dependent eye; down-side shoulder/hip | Axillary roll (chest roll distal to axilla — NOT in axilla); pillows between knees; head neutral; “bean bag” or lateral positioners; pad fibular head | Thoracic, renal, hip, shoulder |
| Sitting (Beach Chair / Fowler’s) | Venous air embolism (VAE) — open veins above heart level; hypotension; sciatic nerve (hip flexion); cervical spine injury during head positioning | Monitor for VAE (precordial Doppler, EtCO₂ drop); flex head carefully; SCDs; careful blood pressure management | Posterior fossa craniotomy, shoulder (beach chair), ENT |
| Kidney / Flank | Brachial plexus; lateral femoral cutaneous nerve; IVC compression; vena caval compression causing hypotension when kidney rest elevated | Kidney rest raised gradually; monitor BP; flex table at iliac crest; axillary roll; all bony prominences padded | Nephrectomy, ureteroscopy, renal surgery |
13. Physiology Concepts Critical to OR Practice
13A. Homeostasis & Fluid/Electrolyte Balance
- Homeostasis — maintenance of stable internal environment; disrupted by surgery (blood loss, fluid shifts, temperature changes, anesthetic effects)
- Sodium (Na⁺) — primary extracellular cation; controls osmolality and water distribution; hyponatremia (<135) → neurological symptoms; hypernatremia (>145) → dehydration
- Potassium (K⁺) — primary intracellular cation; critical for cardiac conduction; hypokalemia → arrhythmias, muscle weakness; hyperkalemia → peaked T waves, cardiac arrest; succinylcholine raises K⁺
- Calcium (Ca²⁺) — muscle contraction, nerve transmission, coagulation; hypocalcemia → tetany, perioral numbness, Chvostek’s sign (facial nerve tapping → facial twitch), Trousseau’s sign; risk after thyroid/parathyroid surgery
- pH / Acid-Base — normal arterial pH 7.35–7.45; acidosis <7.35 (respiratory: ↑CO₂; metabolic: ↓HCO₃); alkalosis >7.45 (respiratory: ↓CO₂; metabolic: ↑HCO₃)
13B. Hemostasis & Coagulation
- Primary hemostasis — vascular spasm → platelet adhesion (vWF bridges collagen and platelets) → platelet aggregation → platelet plug
- Secondary hemostasis (coagulation cascade) — intrinsic pathway (factors XII, XI, IX, VIII — measured by PTT) + extrinsic pathway (tissue factor + VII — measured by PT/INR) → common pathway (X, V, II, I) → thrombin → fibrin clot
- PT/INR — measures extrinsic pathway; elevated in warfarin use, liver disease; goal INR <1.5 before elective surgery
- PTT (aPTT) — measures intrinsic pathway; used to monitor heparin; normal 25–35 sec; therapeutic heparin: 60–100 sec
- Platelets — normal 150,000–400,000/µL; <50,000 = surgical bleeding risk; <20,000 = spontaneous bleeding risk
- Fibrinolysis — plasmin breaks down fibrin; antifibrinolytics (tranexamic acid, aminocaproic acid) prevent this; used to reduce blood loss in major surgery
13C. Thermoregulation
- Normal body temperature: 36.5–37.5°C (97.7–99.5°F); controlled by hypothalamus
- Perioperative hypothermia (<36°C) — most common thermal complication of surgery; causes: cold OR, open body cavities, cold IV fluids, anesthetic-induced vasodilation and impaired thermoregulation
- Consequences of hypothermia: Impaired coagulation, wound infection (impaired neutrophil function), cardiac arrhythmias, increased anesthetic requirements, prolonged drug metabolism, shivering (increased O₂ demand)
- Prevention: Forced-air warming blankets (Bair Hugger); warm IV fluids; warm irrigation; head covering; minimize patient exposure; OR temperature ≥68°F (20°C)
- Hyperthermia in OR — infection, transfusion reaction, malignant hyperthermia (see Pharmacology section); fever >38.3°C postoperatively within first 24 hrs likely from atelectasis or physiologic response, not infection
13D. Shock — Types & Physiological Response
| Type | Mechanism | Signs | Treatment Principle |
|---|---|---|---|
| Hypovolemic | ↓ blood volume (hemorrhage, fluid loss) | ↑HR, ↓BP, pale/cool/clammy skin, ↓UO | Control hemorrhage; IV fluids/blood products |
| Distributive | Vasodilation → relative hypovolemia (sepsis, anaphylaxis, neurogenic) | Warm/flushed skin (sepsis/anaphylaxis); ↓BP; ↑HR | Vasopressors; epinephrine (anaphylaxis); antibiotics (sepsis) |
| Cardiogenic | Pump failure (MI, heart failure, dysrhythmia) | ↓BP, ↑HR, crackles, ↑JVD, ↓CO | Inotropes; IABP; treat arrhythmia; careful fluids |
| Obstructive | Mechanical block to circulation (tension pneumothorax, cardiac tamponade, PE) | Beck’s triad (tamponade: ↓BP, ↑JVD, muffled heart sounds); ↓BP, ↑HR | Remove obstruction: needle decompression (pneumo), pericardiocentesis (tamponade), embolectomy (PE) |
13E. Blood Products
| Product | Contents | Indication | Notes |
|---|---|---|---|
| pRBC (Packed Red Blood Cells) | RBCs; Hgb/Hct; small plasma volume | Anemia; hemorrhage; Hgb <7–8 g/dL typically | 1 unit raises Hgb ~1 g/dL; must be ABO-compatible; infuse through blood filter with NS only |
| FFP (Fresh Frozen Plasma) | All clotting factors + fibrinogen + albumin | Coagulopathy; warfarin reversal; massive transfusion | Must be ABO-compatible; thaw before use; given for elevated PT/INR or PTT; 1 unit raises coagulation factors ~5% |
| Platelets | Platelets in plasma | Thrombocytopenia (<50,000 for surgery); platelet dysfunction | 1 apheresis unit raises count ~50,000; room temperature storage (5 days); agitated to prevent clumping |
| Cryoprecipitate | Fibrinogen, Factor VIII, vWF, Factor XIII | Fibrinogen deficiency, DIC, hemophilia A, vWD | High fibrinogen per volume; pooled; given when fibrinogen <100–150 mg/dL; 10-unit pool is standard |
| Albumin | Colloid protein | Hypoalbuminemia; volume expansion; paracentesis replacement | 5% (iso-oncotic) or 25% (hyper-oncotic); no blood type required; expensive |
14. CST Exam Strategy — A&P Edition
How A&P Appears on the CST Exam
A&P is rarely tested in isolation on the CST exam. Instead, it is embedded in questions about:
- Surgical procedures — “Which structure is most at risk during a thyroidectomy?” → Recurrent laryngeal nerve
- Patient positioning — “Which nerve is most commonly injured in lithotomy position?” → Common peroneal nerve
- Instrumentation & retractors — you must know what structures are being retracted
- Pathology identification — “What organ was resected?” requires knowing anatomy
- Complications — “A patient develops hoarseness postoperatively after a neck dissection — which nerve was injured?” → Recurrent laryngeal (vagus)
Top Tips for A&P on the CST Exam
- Know your at-risk nerves by procedure: Facial nerve (parotid/mastoid); RLN (thyroid/esophageal); brachial plexus (supine/lateral); peroneal nerve (lithotomy). These appear repeatedly.
- Memorize organ locations by quadrant: Know which RUQ/LUQ/RLQ/LLQ organs to identify what surgery is being performed based on incision location.
- Know blood flow through the heart perfectly: Questions about cardiac surgery require knowing the sequence of chambers and valves.
- Master the layers of the abdomen: Skin → fat → fascia → muscle → peritoneum → organ. Every abdominal case closes in reverse. Know what you’re counting in sponge counts.
- Understand dermatomes for spinal anesthesia: T4 = nipples; T10 = umbilicus. A spinal block to T4 is needed for cesarean section.
- Know the right bronchus rule: Right main bronchus is shorter, wider, and more vertical — this is why foreign body aspiration and inadvertent right mainstem intubation occur here.
- Know the ureter trick: Ureters pass under the uterine artery during hysterectomy (“water under the bridge”) — most common site of ureteral injury during GYN surgery.
- Triangles matter: Triangle of Calot (cholecystectomy) → cystic artery identification. Femoral triangle (inguinal surgery) → femoral nerve, artery, vein, lymphatics (NAVEL from lateral to medial).
- Coagulation pathways on the exam: PT/INR = extrinsic = warfarin; PTT = intrinsic = heparin. This is always tested.
- Body cavities and incisions: Know which incision provides access to which cavity. Midline = widest abdominal access; Pfannenstiel = pelvic/GYN; McBurney’s = appendix.
⚡ High-Yield A&P Quick Reference Cards
Heart Valves — Mnemonic
“Try Pulling My Aorta”
Tricuspid (right AV) → Pulmonic → Mitral (left AV) → Aortic
AV valves open during diastole; Semilunar valves open during systole.
Cranial Nerve Mnemonic
“Oh Oh Oh To Touch And Feel Very Good Velvet — Ah Heaven!”
I Olfactory, II Optic, III Oculomotor, IV Trochlear, V Trigeminal, VI Abducens, VII Facial, VIII Vestibulocochlear, IX Glossopharyngeal, X Vagus, XI Accessory, XII Hypoglossal
Femoral Triangle — NAVEL
Lateral → Medial:
Nerve (femoral) | Artery (femoral) | Vein (femoral) | Empty space | Lymphatics
Key for inguinal hernia, femoral access, groin dissection.
Coagulation Labs
PT/INR = Extrinsic pathway = Warfarin effect → factors II, VII, IX, X
PTT/aPTT = Intrinsic pathway = Heparin monitoring
Platelets = Primary hemostasis; <50,000 = surgical bleeding risk
Right vs. Left Bronchus
Right bronchus: shorter, wider, more vertical → foreign body aspiration and inadvertent endobronchial intubation occur here. Right lung has 3 lobes; Left has 2 (room for heart).
Dermatome Landmarks
T4 = Nipple line (spinal level needed for C-section)
T10 = Umbilicus
L4 = Knee
S3–S5 = Perineum/saddle area
C3–C5 = Diaphragm (“phrenic nerve keeps diaphragm alive”)
Abdominal Layers (Outside → In)
Skin → Subcutaneous fat (Camper’s / Scarpa’s fascia) → External oblique → Internal oblique → Transversus abdominis → Transversalis fascia → Preperitoneal fat → Peritoneum → Organ
Most Common Positioning Injury
Common peroneal (fibular) nerve at fibular head — lithotomy/lateral position.
Injury = foot drop (cannot dorsiflex).
Always pad lateral knee and fibular head.
Cushing’s Triad (↑ICP)
↑ Blood Pressure + ↓ Heart Rate + Irregular Respirations = Brain herniation warning. Notify surgeon immediately. Treat with mannitol, hyperventilation, HOB elevation.
Structures at Risk by Surgery
Thyroidectomy: RLN, parathyroids
Parotidectomy: Facial nerve (CN VII)
Hysterectomy: Ureters (“water under the bridge”)
CEA: Hypoglossal, vagus nerves
Cholecystectomy: Common bile duct
Beck’s Triad — Cardiac Tamponade
↓ Blood pressure + ↑ JVD (jugular venous distension) + Muffled heart sounds
Treatment: pericardiocentesis (needle aspiration of pericardial sac) or surgical pericardial window.
Appendix / McBurney’s Point
Located at 1/3 distance from the ASIS to the umbilicus in the RLQ. Appendix attaches to base of cecum. Classic appendicitis: pain starts periumbilical → migrates to McBurney’s point.
© 2026 Coy Academy. All rights reserved. No part of this material may be reproduced or transmitted in any form or by any means without the prior written permission of Coy Academy.