Microbiology is one of the highest-yield basic science topics on the CST exam. This lesson condenses a full semester of microbiology into the core concepts you must know — organized exactly the way the exam tests them.
1. Classification of Microorganisms
Microorganisms are classified based on their structure, reproduction, and pathogenic potential. The five major groups tested on the CST exam are bacteria, viruses, fungi, parasites, and prions.
1A. Bacteria
Bacteria are prokaryotic (no nucleus), single-celled organisms that reproduce by binary fission. They are classified by:
- Shape: Coccus (sphere), Bacillus (rod), Spirillum/Spirochete (spiral), Vibrio (comma-shaped)
- Gram stain: Gram-positive (purple — thick peptidoglycan wall) vs. Gram-negative (pink/red — thin wall + outer lipopolysaccharide membrane)
- Oxygen requirement: Aerobic, anaerobic, facultative anaerobe, microaerophilic
- Spore formation: Endospores resist heat, chemicals, and drying (e.g., Clostridium, Bacillus)
| Organism | Gram | Shape | Disease / OR Relevance |
|---|---|---|---|
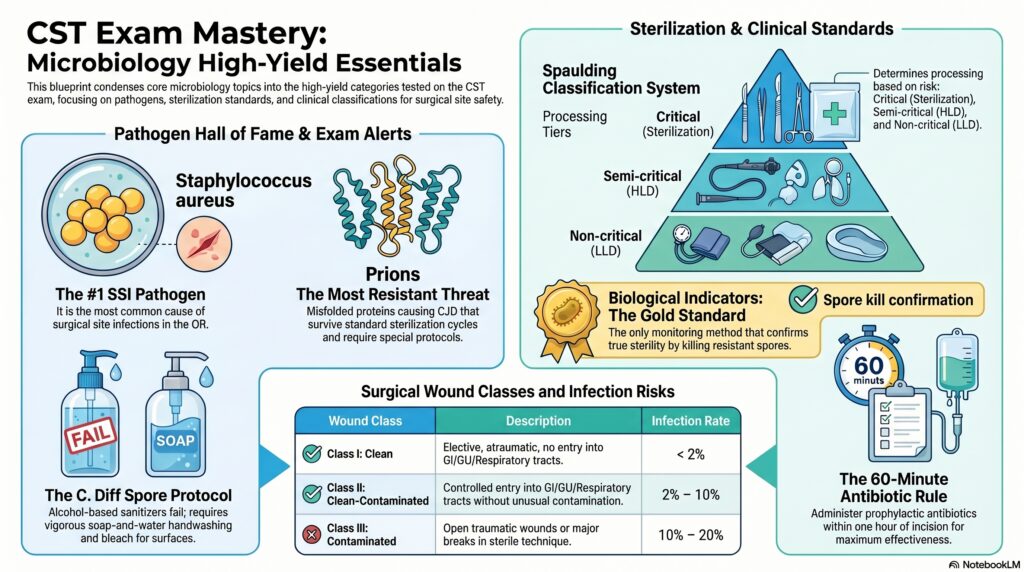
| Staphylococcus aureus | + | Coccus (clusters) | Most common SSI pathogen, MRSA, is a major HAI concern |
| Streptococcus pyogenes | + | Coccus (chains) | Necrotizing fasciitis, wound infections |
| Clostridium perfringens | + | Bacillus | Gas gangrene; anaerobe; spore-former |
| Clostridium tetani | + | Bacillus | Tetanus; “drumstick” spore; anaerobe |
| Clostridium difficile (C. diff) | + | Bacillus | Post-antibiotic colitis; spores resist alcohol-based hand sanitizers |
| Pseudomonas aeruginosa | − | Bacillus | Burn/wound infections; blue-green pigment; highly antibiotic-resistant |
| Escherichia coli | − | Bacillus | UTI, bowel surgery contamination |
| Mycobacterium tuberculosis | Acid-fast | Bacillus | TB; requires Airborne Precautions; N95 mask |
| Treponema pallidum | Not Gram-stainable | Spirochete | Syphilis; blood/body fluid precautions |
1B. Viruses
Viruses are non-cellular obligate intracellular parasites — they cannot replicate without a host cell. They contain either DNA or RNA (never both), surrounded by a protein coat called a capsid, and some have a lipid envelope.
- Enveloped viruses (HIV, HBV, HCV, Influenza, CMV, HSV, EBV) — easier to destroy; killed by soap/detergent
- Non-enveloped viruses (Norovirus, Adenovirus, HAV, Parvovirus) — more resistant to disinfectants
| Virus | Type | Transmission | OR / Precaution Note |
|---|---|---|---|
| HIV | RNA retrovirus | Blood/body fluids, sexual contact | Standard Precautions; double-glove; needlestick protocol |
| Hepatitis B (HBV) | DNA virus | Blood/body fluids; most infectious bloodborne pathogen | Vaccine available; can survive on surfaces 7+ days |
| Hepatitis C (HCV) | RNA virus | Blood (needlestick most common in OR) | No vaccine; leading cause of liver transplant |
| Herpes Simplex (HSV) | DNA virus | Direct contact with lesions | Herpetic whitlow risk for OR staff |
| Norovirus | RNA non-enveloped | Fecal-oral; very low infectious dose | Contact + Droplet; soap & water (not hand sanitizer alone) |
| Influenza | RNA virus | Droplets | Droplet Precautions; annual vaccination recommended |
1C. Fungi
Fungi are eukaryotic organisms with a cell wall made of chitin (not peptidoglycan). They can exist as yeasts (unicellular), molds (multicellular hyphae), or dimorphic (both forms).
- Candida albicans — most common fungal SSI; opportunistic; forms pseudohyphae; causes oral thrush and wound infections in immunocompromised patients
- Aspergillus fumigatus — airborne mold; dangerous in OR (air filtration critical); causes invasive aspergillosis in immunocompromised
- Cryptococcus neoformans — encapsulated yeast; associated with pigeon droppings; meningitis in AIDS patients
- Dermatophytes (Tinea species) — superficial infections (ringworm, athlete’s foot, jock itch)
1D. Parasites
- Protozoa (unicellular eukaryotes): Plasmodium (malaria — mosquito vector), Toxoplasma gondii (cat feces; risk in pregnancy), Giardia lamblia (fecal-oral; cysts in water)
- Helminths (worms): Taenia spp. (tapeworms), Ascaris lumbricoides (roundworm), Enterobius vermicularis (pinworm)
- Ectoparasites: Lice (Pediculus), Scabies (Sarcoptes scabiei) — Contact Precautions
1E. Prions
Prions are misfolded proteins with no DNA or RNA. They cause fatal neurodegenerative diseases such as Creutzfeldt-Jakob Disease (CJD). Prions are extraordinarily resistant — they are NOT destroyed by standard sterilization (steam, EtO, formaldehyde, or radiation). Special protocols include extended gravity steam cycles (134°C for 18 min) or 1N NaOH immersion. Instruments used on suspected prion patients are typically quarantined or destroyed.
2. Microbial Characteristics & Terminology
| Term | Definition |
|---|---|
| Pathogen | An organism capable of causing disease |
| Virulence | Degree of pathogenicity: ability to cause disease |
| Toxin | Poisonous substance produced by microorganism; exotoxin = secreted by living bacteria (e.g., C. tetani); endotoxin = LPS released when Gram-negative bacteria die (causes fever, septic shock) |
| Normal flora | Non-pathogenic organisms that normally inhabit skin, GI tract, etc.; can become opportunistic pathogens when displaced (e.g., surgery) |
| Opportunistic infection | Caused by organisms that are non-pathogenic in a healthy host but cause disease in immunocompromised individuals |
| Biofilm | Community of microbes encased in a polysaccharide matrix; adheres to surfaces (implants, instruments); highly resistant to antibiotics and disinfectants |
| Endospore | Dormant, heat/chemical-resistant structure formed by Clostridium and Bacillus; only destroyed by sterilization (not disinfection) |
| Septicemia / Sepsis | Systemic inflammatory response to infection; bacteria in the bloodstream (bacteremia); life-threatening |
3. The Chain of Infection
Infection requires all six links in the chain. Breaking any single link prevents infection — the foundation of aseptic technique.
① Infectious Agent (Pathogen)
The microorganism itself (bacteria, virus, fungus, parasite, prion). Virulence, quantity, and host susceptibility determine if the disease occurs.
② Reservoir
Where the organism lives and multiplies: humans, animals, soil, water, surgical instruments, and OR surfaces.
③ Portal of Exit
How the organism leaves the reservoir: respiratory secretions, blood, wound drainage, feces, urine, skin shedding.
④ Mode of Transmission
Contact (direct/indirect), Droplet (>5 µm), Airborne (<5 µm droplet nuclei), Vector-borne, Vehicle (food/water/IV fluid)
⑤ Portal of Entry
Broken skin, mucous membranes, respiratory tract, GI tract, GU tract, and surgical incision (the primary OR portal).
⑥ Susceptible Host
Risk factors: age (very young/old), immunosuppression, diabetes, malnutrition, prolonged hospital stay, invasive devices.
4. Transmission-Based Precautions (CDC)
Standard Precautions are used for ALL patients regardless of diagnosis. Transmission-Based Precautions are added on top of Standard Precautions.
| Precaution Type | PPE Required | Common Organisms / Diseases | Room Type |
|---|---|---|---|
| Standard | Gloves, gown (if splash risk), mask/eye protection (if splash risk) | ALL patients | Any |
| Contact | Gloves + Gown (donned on entry) | MRSA, VRE, C. diff, RSV, scabies, wound infections, multi-drug resistant organisms (MDROs) | Private or cohorted |
| Droplet | Surgical mask (within 3–6 ft) | Influenza, Meningococcal meningitis, pertussis, mumps, rubella, pneumonic plague | Private preferred |
| Airborne | N95 respirator (or higher); + negative pressure room | TB (M. tuberculosis), measles (rubeola), varicella (chickenpox), SARS, monkeypox (airborne component) | Negative pressure, air-handling 6–12 ACH |
5. Sterilization, Disinfection & Antisepsis
5A. Spaulding Classification
The Spaulding system classifies medical devices by infection risk to determine the required level of processing:
| Category | Definition | Required Processing | Examples |
|---|---|---|---|
| Critical | Enters sterile tissue or vascular system | Sterilization | Scalpels, needles, implants, surgical instruments |
| Semi-critical | Contacts mucous membranes or non-intact skin | High-Level Disinfection (minimum) | Endoscopes, laryngoscope blades, respiratory equipment |
| Non-critical | Contacts intact skin only | Low- or Intermediate-Level Disinfection | Blood pressure cuffs, stethoscopes, OR furniture, floors |
5B. Levels of Germicidal Activity
| Level | Kills | Examples |
|---|---|---|
| Sterilization | ALL microorganisms, including spores | Steam autoclave, EtO gas, plasma (H₂O₂), dry heat, radiation |
| High-Level Disinfection (HLD) | All except large numbers of bacterial spores | Glutaraldehyde 2%, ortho-phthalaldehyde (OPA), peracetic acid, hydrogen peroxide >6% |
| Intermediate-Level Disinfection | Vegetative bacteria, mycobacteria, most viruses and fungi; NOT spores | EPA-registered tuberculocidal disinfectants, iodophors, phenolics, 70% isopropyl alcohol |
| Low-Level Disinfection | Most bacteria, some fungi, some viruses; NOT mycobacteria or spores | Quaternary ammonium compounds (quats), dilute bleach, and some phenolics |
5C. Sterilization Methods
| Method | Parameters | Advantages / Limitations |
|---|---|---|
| Steam Autoclave (Moist Heat) | Gravity: 250°F (121°C) / 15–30 min Prevacuum: 270°F (132°C) / 4 min |
Gold standard; fast; inexpensive; cannot use on heat- or moisture-sensitive items |
| Ethylene Oxide (EtO) Gas | Low temperature; 10–16 hr cycle including aeration | For heat/moisture-sensitive items (cameras, plastics, rubber); toxic/carcinogenic gas; long cycle; requires aeration |
| Hydrogen Peroxide Plasma (STERRAD®) | Low temperature; ~55°C; 28–75 min | Rapid; safe (no toxic residues); for scopes/electronics; cannot use with cellulose-based items (linen, paper) |
| Dry Heat | 160–170°C / 1–2 hr | For items that cannot be moistened (powders, oils, anhydrous materials) |
| Peracetic Acid (STERIS®) | Liquid immersion; 50–55°C; 12 min | For heat-sensitive rigid scopes, no drying time; must be used immediately (no storage in sterile state) |
| Immediate-Use Steam Sterilization (IUSS / Flash) | 132°C gravity; unwrapped; 3 min (non-porous items) | Emergency use only — dropped instrument, no backup available; items cannot be stored; documentation required; not routine sterilization method |
5D. Sterilization Monitoring
| Monitor Type | What It Tests | Examples / Notes |
|---|---|---|
| Mechanical / Physical | Equipment function — pressure, temperature, time printouts | Reviewed each cycle; logged |
| Chemical Indicators (CI) | Exposure to sterilant (NOT sterility) | Class 1–6 indicators; autoclave tape (Class 1); Bowie-Dick test (Class 2); integrators (Class 5) |
| Biological Indicators (BI) | Gold standard — actual killing of resistant spores; confirms true sterility | Steam: Geobacillus stearothermophilus; EtO/dry heat: Bacillus atrophaeus; Run weekly minimum (daily for IUSS); results in 24–48 hr (rapid BI in 1 hr) |
6. Surgical Site Infections (SSIs) & Wound Classification
6A. CDC Wound Classification
| Class | Description | Infection Rate | Examples |
|---|---|---|---|
| Class I — Clean | Elective, atraumatic, no inflammation, no break in aseptic technique, respiratory/GI/GU tract not entered | <2% | Hernia repair, thyroidectomy, hip replacement |
| Class II — Clean-Contaminated | Controlled entry into GI, GU, respiratory tract without unusual contamination | 2–10% | Cholecystectomy, bowel resection with bowel prep, hysterectomy |
| Class III — Contaminated | Open, fresh traumatic wounds; major breaks in technique; gross spillage from GI tract; acute non-purulent inflammation | 10–20% | Penetrating abdominal trauma, rectal surgery with fecal spillage |
| Class IV — Dirty/Infected | Old traumatic wounds, purulent infection, perforated viscus present preoperatively | >20–40% | Ruptured appendix with abscess, debridement of infected wound |
6B. SSI Classification (CDC Definitions)
- Superficial Incisional SSI — involves skin and subcutaneous tissue; occurs within 30 days; signs: redness, swelling, pain, purulent drainage
- Deep Incisional SSI — involves deep soft tissues (fascia, muscle); within 30–90 days; fever, wound dehiscence, purulent drainage from depth
- Organ/Space SSI — involves any organ or space manipulated during surgery (e.g., intra-abdominal abscess, empyema); within 30–90 days
6C. Risk Factors for SSI
Patient Factors
- Diabetes/hyperglycemia
- Obesity (BMI >30)
- Smoking / poor oxygenation
- Immunosuppression (steroids, chemo)
- Malnutrition/hypoalbuminemia
- MRSA colonization
- Prolonged preoperative hospital stay
Operative / System Factors
- Prolonged operative time
- Inadequate skin prep
- Break in aseptic technique
- Hypothermia during surgery
- Excessive tissue trauma / dead space
- Foreign body (drains, implants)
- Shaving (vs. clipping) hair
6D. SSI Prevention Bundle
- Preoperative antibiotic prophylaxis — administered within 60 minutes before incision (120 min for vancomycin/fluoroquinolones); re-dosed for long cases (>4 hrs or major blood loss)
- Skin antisepsis — Chlorhexidine-alcohol preferred for most sites; iodine-alcohol for head/face; allow to dry/off-gas before draping
- Hair removal — clip (never shave) immediately preoperatively if necessary; shaving increases SSI risk via microabrasions
- Normothermia — maintain patient temperature >36°C; hypothermia impairs neutrophil function and vasoconstriction reduces tissue O₂
- Glucose control — maintain perioperative blood glucose <200 mg/dL (hyperglycemia impairs phagocytosis)
- MRSA decolonization — nasal mupirocin + chlorhexidine baths preoperatively in known carriers
- Maintain sterile technique — strict adherence to aseptic principles throughout the procedure
7. Principles of Asepsis & Aseptic Technique
7A. AORN / AST Principles of Aseptic Technique
- Only sterile items are used within the sterile field. If questionable — consider it contaminated.
- Sterile persons are gowned and gloved. Gown is sterile from chest to waist in front; 2 inches above elbow to cuff; back is not considered sterile.
- Sterile persons touch only sterile items or areas; unsterile persons touch only unsterile items.
- Unsterile persons avoid reaching over the sterile field.
- The edges of sterile packages/containers are not sterile. A 1-inch perimeter of sterile drapes is considered contaminated.
- The sterile field is always within vision and above the waist level. Items below the table level are contaminated.
- Contamination is recognized and corrected immediately.
- Sterile barriers that have been permeated must be considered contaminated. Wet/strike-through = contaminated.
- Movement around the sterile field must not contaminate it. Sterile persons pass back-to-back; unsterile face away.
- The sterile field is prepared as close to the time of use as possible.
7B. Skin Antiseptics for Surgical Prep
| Agent | Spectrum | Notes / Contraindications |
|---|---|---|
| Chlorhexidine gluconate (CHG) | Broad-spectrum; G+, G−, fungi, some viruses | Persistent activity (residual effect); avoid on ears/eyes (ototoxic); most common choice for skin prep |
| Povidone-Iodine (Betadine) | Broad-spectrum; bactericidal, sporicidal, virucidal, fungicidal | Must dry to be effective; avoid on thyroid patients (iodine absorption); stains; protein-inactivated |
| Isopropyl Alcohol (70%) | Bactericidal, virucidal, fungicidal; NOT sporicidal | Must fully dry/off-gas before draping or using electrosurgery — fire risk; no residual activity |
| Hexachlorophene | Primarily G+ (poor G−) | Neurotoxic; no longer used for skin prep; historical context only |
7C. Surgical Hand Scrub / Rub
- Traditional scrub — antiseptic soap (CHG or iodine-based); timed or counted-stroke method; fingernails to 2 inches above elbow; nailpick used for subungual debris on first scrub of day
- Brushless surgical hand rub (antiseptic rub) — CHG or alcohol-based; approved as equivalent to traditional scrub; must perform initial hand wash first; apply per manufacturer’s instructions until dry
- Goal — reduce resident and transient flora to as close to zero as possible; maintain bacteriostatic effect throughout procedure
8. Healthcare-Associated Infections (HAIs) & MDROs
HAIs are infections acquired in a healthcare setting, not present or incubating at admission. Major categories relevant to the OR:
| HAI Type | Common Pathogens | Prevention |
|---|---|---|
| Surgical Site Infection (SSI) | S. aureus/MRSA, E. coli, Pseudomonas, Klebsiella | Antibiotic prophylaxis, skin prep, sterile technique |
| Central Line-Associated Bloodstream Infection (CLABSI) | S. epidermidis, S. aureus, Candida | Central line bundle: hand hygiene, max barrier, CHG prep, optimal site, daily necessity review |
| Catheter-Associated UTI (CAUTI) | E. coli, Enterococcus, Pseudomonas, Candida | Remove catheter ASAP; sterile insertion; closed drainage system |
| Ventilator-Associated Pneumonia (VAP) | Pseudomonas, S. aureus, Acinetobacter | HOB elevation 30–45°, oral care, hand hygiene, sedation vacation |
8A. Multi-Drug Resistant Organisms (MDROs)
| Organism | Resistance | Precautions |
|---|---|---|
| MRSA (Methicillin-Resistant S. aureus) | Resistant to all beta-lactams; treat with Vancomycin | Contact Precautions |
| VRE (Vancomycin-Resistant Enterococcus) | Resistant to vancomycin; treat with linezolid or daptomycin | Contact Precautions |
| CRE (Carbapenem-Resistant Enterobacteriaceae) | Resistant to carbapenems (last-resort antibiotics); extremely dangerous | Contact Precautions; enhanced environmental cleaning |
| ESBL producers (E. coli, Klebsiella) | Extended-spectrum beta-lactamase; resistant to most penicillins/cephalosporins | Contact Precautions; carbapenem treatment |
9. Wound Healing
9A. Types of Wound Healing
- Primary intention (first intention) — wound edges approximated (sutured); minimal scarring; clean wounds; fastest healing
- Secondary intention — wound left open to heal by granulation tissue formation; used for infected/contaminated wounds; more scarring; slower
- Tertiary intention (delayed primary closure) — wound initially left open (class III/IV), then closed 4–5 days later after infection resolves; combines features of both
9B. Phases of Wound Healing
| Phase | Timing | Key Events |
|---|---|---|
| Inflammatory | Days 1–4 | Hemostasis (clot formation), vasodilation, neutrophil influx, macrophage activity (debridement), signs of inflammation (rubor, calor, dolor, tumor) |
| Proliferative | Days 5–20 | Fibroblast activity, collagen synthesis, angiogenesis (new blood vessel formation), granulation tissue, wound contraction, epithelialization |
| Remodeling / Maturation | Day 21 – up to 2 years | Collagen remodeling (type III → type I); scar formation; max wound tensile strength ~80% of original; hypertrophic scars vs. keloids |
9C. Halsted’s Principles of Wound Healing
These surgical principles minimize tissue trauma and infection, promoting optimal healing:
- Gentle handling of tissues
- Meticulous hemostasis
- Preservation of the blood supply
- Strict aseptic technique
- Minimal use of sutures and foreign bodies
- Obliteration of dead space
- Tension-free wound approximation
9D. Complications of Wound Healing
- Dehiscence — wound separation, most common around post-op day 5; risk: obesity, infection, poor nutrition, steroid use
- Evisceration — protrusion of abdominal organs through the wound; surgical emergency; cover with sterile saline-moistened towel, return to OR immediately
- Hematoma — collection of blood in a wound; risk for infection; inadequate hemostasis
- Seroma — collection of serous fluid; common after mastectomy, axillary dissection
- Keloid — hypertrophic scar that extends beyond wound margins; more common in darker-pigmented skin
- Fistula — abnormal connection between two epithelialized surfaces; can result from infection or poor healing
10. Surgical Specimen Handling
Proper specimen handling is both a microbiology and patient safety concern. The scrub technologist plays a key role:
- Chain of custody — all specimens must be labeled immediately (patient name, MRN, date/time, specimen site, laterality) and accompanied by completed requisition
- Fresh/unfixed — sent immediately to pathology without preservative; used for frozen section (intraoperative pathology), flow cytometry, cultures
- Formalin (10% neutral buffered formalin) — most common fixative for permanent histology; tissue:formalin ratio 1:10; do NOT use for cultures (kills bacteria)
- Culture specimens — placed in appropriate culture medium (aerobic, anaerobic, fungal, mycobacterial); swab or tissue in transport media; deliver promptly to lab
- Frozen section — rapid intraoperative diagnosis (15–20 min); determines surgical margins and guides extent of resection
- Calculi / foreign bodies — dry container; no formalin; sent for analysis, not pathology
- Amputated limbs — wrapped in saline-moistened towel and plastic bag; labeled; transported per institutional policy
11. The Immune System & Host Defenses
11A. Lines of Defense
- 1st Line (Physical/Chemical Barriers) — intact skin, mucous membranes, cilia, stomach acid (pH 2), lysozyme in tears/saliva, normal flora competition
- 2nd Line (Innate/Non-specific Immunity) — inflammation, fever, phagocytes (neutrophils, macrophages), natural killer (NK) cells, complement system, interferons
- 3rd Line (Adaptive/Specific Immunity) — T lymphocytes (cell-mediated), B lymphocytes → plasma cells → antibodies (humoral); immunological memory (vaccination basis)
11B. Immunity Types
| Type | How Acquired | Example |
|---|---|---|
| Active Natural | Having the disease and recovering | Chickenpox infection → lifelong immunity |
| Active Artificial | Vaccination | Hepatitis B vaccine, MMR, influenza vaccine |
| Passive Natural | Maternal antibodies transferred to fetus/infant | IgG across placenta; IgA in breast milk |
| Passive Artificial | Injection of preformed antibodies (immune globulin) | Tetanus immune globulin (TIG), Hepatitis B immune globulin (HBIG) |
12. Bloodborne Pathogens & OSHA Standards
The OSHA Bloodborne Pathogen Standard (29 CFR 1910.1030) mandates protection for all healthcare workers exposed to blood and OPIM (Other Potentially Infectious Materials).
Key Bloodborne Pathogens in the OR
| Pathogen | Risk per Needlestick | Vaccine Available? | Post-Exposure Action |
|---|---|---|---|
| HBV | 6–30% (highest) | Yes (3-dose series) | HBIG + vaccine if unvaccinated; report within 24 hrs |
| HCV | 1.8% average | No | Baseline testing, monitor, and treat if seroconversion |
| HIV | 0.3% percutaneous; 0.09% mucosal | No | PEP (post-exposure prophylaxis) within 2 hrs; 28-day regimen |
Sharps Safety in the OR
- Neutral zone / hands-free technique — scalpels, needles, and sharp instruments are placed in a designated area (basin, magnetic pad) on the sterile field rather than passed hand-to-hand
- No two-hand recapping — single-hand scoop or safety device only
- Sharps count — all sharps counted before, during (when cavity opened), and after procedure
- Sharps disposal — puncture-resistant containers; do not overfill (>3/4 full)
- Double gloving — reduces perforation exposure; inner glove perforations often undetected without double gloving
13. Microbiology of the OR Environment
- Air quality — OR maintained at positive pressure relative to corridors (except airborne isolation ORs); HEPA filtration; minimum 15–20 air changes per hour (ACH); ultraclean rooms for implants may use laminar airflow (>400 ACH)
- Temperature and humidity — OR temperature 68–75°F (20–24°C); relative humidity 30–60%; low humidity increases static electricity and particulate dispersal; high humidity promotes microbial growth
- OR traffic — each time OR door opens, positive pressure disruption and airborne contamination increase; minimize traffic and door openings during procedures
- Environmental cleaning — wet mopping (damp, not dry — dry dusting disperses particles); OR cleaned between cases and at end of day with EPA-registered disinfectant; terminal cleaning weekly
- Sources of contamination in the OR — personnel (primary source — skin squames, respiratory droplets), patient’s own flora, instruments, environment
- Surgical attire — scrub suit, head covering (all hair covered), shoe covers; masks worn in semi-restricted/restricted areas; jewelry removed; artificial nails and nail polish prohibited (harbor bacteria)
14. Antibiotics & Antimicrobial Agents
Know the mechanism, coverage, and surgical relevance of major antibiotic classes:
| Class | Mechanism | Coverage / Examples | Surgical Relevance |
|---|---|---|---|
| Penicillins | Inhibit cell wall synthesis (beta-lactam ring) | G+; ampicillin, amoxicillin, oxacillin | Allergy risk; cross-reactivity with cephalosporins (10%) |
| Cephalosporins | Cell wall synthesis inhibition (beta-lactam) | Broad; cefazolin (1st gen) = most common prophylaxis; 4th gen = Pseudomonas | Cefazolin is the #1 surgical prophylaxis antibiotic |
| Vancomycin | Cell wall synthesis inhibition (glycopeptide) | G+ including MRSA; not G− | “Red man syndrome” if infused too fast; used for MRSA-colonized patients pre-op; infuse over 60–120 min; start 120 min before incision |
| Aminoglycosides | Inhibit protein synthesis (30S ribosome) | G− aerobes; gentamicin, tobramycin, amikacin | Nephrotoxic + ototoxic; monitor drug levels; can be irrigated into wounds |
| Metronidazole (Flagyl) | Disrupts DNA synthesis | Anaerobes + protozoa; colorectal surgery prophylaxis (with cephalosporin) | No alcohol during/after treatment; covers C. diff treatment |
| Fluoroquinolones | Inhibit DNA gyrase/topoisomerase IV | Broad G+ and G−; ciprofloxacin, levofloxacin | Risk of tendon rupture; 120 min pre-op window for prophylaxis |
| Antifungals | Target ergosterol in fungal cell membrane | Fluconazole (Candida); amphotericin B (severe systemic); nystatin (topical) | Amphotericin B nephrotoxic; used for invasive fungal infections in immunocompromised |
⚡ High-Yield Exam Quick Reference
Gram Stain Memory Aid
G+ = Purple = Positive = Pretty thick wall
G− = Red/Pink = Negative = Nasty outer membrane (LPS → endotoxin)
Sterilization Hierarchy
Steam autoclave → EtO/H₂O₂ Plasma → Dry heat → Liquid chemical sterilants
Only biological indicators confirm true sterilization.
#1 SSI Pathogen
Staphylococcus aureus (especially MRSA)
The most common causative organism of surgical site infections.
Airborne vs. Droplet
Airborne (<5 µm): TB, measles, varicella → N95 + negative pressure
Droplet (>5 µm): Flu, meningitis → surgical mask
Prophylactic Antibiotic Rule
Cefazolin within 60 minutes of incision (Vancomycin/FQ: 120 min). Redose if >4 hrs or major blood loss. D/C within 24 hrs post-op.
Spore-Formers to Know
Clostridium perfringens (gas gangrene)
Clostridium tetani (tetanus)
Clostridium difficile (colitis — use soap, not sanitizer)
Bacillus anthracis (anthrax)
Flash Sterilization (IUSS)
Emergency use only. Unwrapped, 132°C, 3 min gravity (non-porous). No storage. Document reason. Never routine.
Prion Special Protocol
Standard sterilization does NOT destroy prions. CJD instruments: quarantine or destroy. Extended steam (134°C/18 min) or 1N NaOH if processing required.
Wound Class → Infection Risk
I Clean <2% | II Clean-Contaminated 2–10% | III Contaminated 10–20% | IV Dirty >20%
HBV is the Most Infectious BBP
HBV: 6–30% per needlestick (highest). HCV: ~1.8%. HIV: 0.3%. HBV survives on surfaces 7+ days. Vaccine available for HBV only.
Alcohol Skin Prep — Fire Risk
Alcohol-based prep (CHG-alcohol, Betadine-alcohol) MUST fully dry/off-gas before draping or activating ESU. Pooling under drapes = surgical fire risk.
Evisceration Management
Surgical emergency. Cover with a sterile saline-moistened towel. Do NOT push organs back in. Keep the patient supine. Notify the surgeon and return to the OR immediately.
© 2024 Coy Academy. All rights reserved. No part of this material may be reproduced or transmitted in any form or by any means without the prior written permission of Coy Academy.