Surgical pharmacology is one of the highest-tested areas on the CST exam. The scrub technologist must understand what drugs are on the sterile field, why they are used, how they are prepared and passed, and what adverse effects to watch for. This lesson condenses a full pharmacology course into everything you need to know for exam day — and for day one in the OR.
1. Pharmacology Fundamentals
1A. Key Terminology
| Term | Definition |
|---|---|
| Pharmacokinetics | What the body does to the drug — Absorption, Distribution, Metabolism, Excretion (ADME) |
| Pharmacodynamics | What the drug does to the body — mechanism of action, receptor interactions, drug effects |
| Onset | Time from administration to first observable therapeutic effect |
| Peak | Time at which drug reaches maximum concentration/effect |
| Duration | Length of time the drug produces a therapeutic effect |
| Half-life (t½) | Time required for drug concentration in the body to decrease by 50% |
| Therapeutic index (TI) | Ratio of toxic dose to therapeutic dose; narrow TI drugs (e.g., heparin, digoxin) require careful monitoring |
| Agonist | Drug that binds to a receptor and activates it (mimics natural ligand) |
| Antagonist | Drug that binds to a receptor and blocks it (reversal agents are often antagonists) |
| Synergism | Combined effect of two drugs is greater than each alone (e.g., opioid + benzodiazepine → enhanced sedation/respiratory depression) |
| Antagonism | One drug reduces or cancels the effect of another |
| Tolerance | Decreased response to a drug over time; requires higher doses for same effect |
| Idiosyncratic reaction | Unexpected, abnormal reaction unique to an individual (not predictable based on pharmacology) |
| Anaphylaxis | Severe, life-threatening allergic reaction; treat with epinephrine immediately |
1B. Routes of Administration
| Route | Description | Onset | OR Examples |
|---|---|---|---|
| Intravenous (IV) | Directly into bloodstream; most common in OR | Seconds–minutes | Propofol, fentanyl, antibiotics, heparin |
| Inhalation | Via respiratory tract; absorbed through alveoli | Seconds–minutes | Volatile anesthetic gases (sevoflurane, desflurane, isoflurane) |
| Topical / Local | Applied to skin or mucous membranes; on sterile field | Minutes | Thrombin, epinephrine-soaked pledgets, topical antibiotics, cocaine (ENT), bacitracin irrigation |
| Subcutaneous (SC/SQ) | Into subcutaneous fat layer | Minutes–hours | Insulin, heparin (DVT prophylaxis), local anesthetics |
| Intramuscular (IM) | Into muscle; slower than IV | 10–30 min | Ketorolac (Toradol), antibiotics, epinephrine auto-injector |
| Intrathecal / Spinal | Into subarachnoid space; CSF distribution | Minutes | Spinal anesthesia (bupivacaine + fentanyl), spinal opioids |
| Epidural | Into epidural space (outside dura); continuous catheter possible | 10–20 min | Epidural anesthesia/analgesia; OB, thoracic, orthopedic cases |
| Intraosseous (IO) | Into bone marrow cavity; emergency access | Seconds–minutes | Pediatric emergencies when IV access unobtainable |
1C. Drug Safety on the Sterile Field
The scrub technologist is responsible for all drugs on the sterile field. Key responsibilities:
- Label ALL medications immediately upon receiving them onto the sterile field — label must include drug name, strength/concentration, and any relevant information (e.g., “with epi” or “without epi”)
- Verify verbally with the circulator: name, dose, concentration, and expiration before use
- Never use unlabeled medications — discard if any doubt exists
- Pass medications to surgeon safely — announce drug name and concentration when passing; do not place on surgeon’s hand without verbal confirmation
- Use a standardized syringe size for each drug type to prevent mix-ups; many facilities use color-coded labels
- Know the difference between “with epinephrine” and “plain” local anesthetics — administering epinephrine inadvertently in certain sites (digits, nose, penis, ears) can cause ischemia and necrosis
2. Anesthesia
2A. Types of Anesthesia
General Anesthesia (GA)
Loss of consciousness, sensation, and reflexes; requires airway management (ETT or LMA). Components: amnesia, analgesia, muscle relaxation, loss of consciousness (the “4 As” — analgesia, amnesia, areflexia, autonomic stability).
Regional Anesthesia
Blocks sensation to a region of the body. Patient may remain awake. Includes spinal, epidural, peripheral nerve blocks. No airway management typically required.
Local Anesthesia
Blocks sensation at the surgical site only; patient is awake. Administered by surgeon or anesthesia provider. Examples: lidocaine, bupivacaine. Frequently on the sterile field.
Monitored Anesthesia Care (MAC)
Anesthesia provider monitors patient while providing IV sedation (often midazolam + fentanyl or propofol). Patient breathes spontaneously. Used for minor procedures, endoscopy, and some orthopedic cases.
Conscious Sedation
Reduced level of consciousness; patient can respond to verbal stimulation; protective reflexes maintained. Used in GI suite, interventional radiology, cardiac cath lab.
Total Intravenous Anesthesia (TIVA)
GA maintained entirely with IV drugs (usually propofol infusion ± opioids/ketamine). No volatile agents. Used when inhalation agents are contraindicated (e.g., malignant hyperthermia risk).
2B. Stages of General Anesthesia (Guedel’s Classification)
| Stage | Name | Characteristics |
|---|---|---|
| I | Induction / Analgesia | Conscious; analgesia present; patient can follow commands; amnesia begins |
| II | Delirium / Excitement | Unconscious; irregular breathing; risk of vomiting, laryngospasm; no procedures during this stage; move quickly through |
| III | Surgical Anesthesia | Surgery can begin; regular respirations; muscle relaxation; further divided into planes (III-1 through III-4) |
| IV | Medullary Depression | Respiratory arrest, circulatory collapse; anesthetic overdose; death if not reversed |
2C. Inhalation (Volatile) Anesthetic Agents
| Agent | Key Properties | Notable Points |
|---|---|---|
| Sevoflurane | Sweet smell; rapid onset/offset; minimal airway irritation | Most common inhalation agent; preferred for inhalation induction (pediatrics); triggers malignant hyperthermia |
| Desflurane | Fastest emergence; pungent; requires heated vaporizer | Used for long cases; airway irritant (coughing, laryngospasm); triggers MH; significant greenhouse gas concerns |
| Isoflurane | Pungent; slower onset/offset; coronary vasodilator | Less common now; triggers MH; caution in coronary artery disease (coronary steal) |
| Nitrous Oxide (N₂O) | Gas at room temperature; analgesic; minimal muscle relaxation | Does NOT trigger MH; expands gas-filled spaces (avoid in bowel obstruction, pneumothorax, middle ear surgery, intracranial air); “laughing gas”; occupational exposure risk |
| Halothane | Older agent; sweet smell; potent | Rarely used; hepatotoxic (halothane hepatitis); triggers MH; sensitizes heart to epinephrine (arrhythmias); largely replaced by newer agents |
2D. IV Induction & Maintenance Agents
| Drug | Class | Uses | Key Notes |
|---|---|---|---|
| Propofol | Alkylphenol | Induction and maintenance (TIVA); MAC sedation | Milky white emulsion (“milk of amnesia”); rapid onset/offset; antiemetic effect; causes pain on injection; hypotension; soy/egg allergy consideration; does NOT trigger MH |
| Ketamine | Dissociative (NMDA antagonist) | Induction (trauma, pediatrics, hemodynamic instability); procedural sedation; analgesia | Maintains airway reflexes and respiratory drive; increases HR, BP (sympathomimetic); causes emergence delirium (hallucinations); bronchodilator; avoid in elevated ICP; does NOT trigger MH |
| Etomidate | Imidazole | Induction in hemodynamically unstable patients | Minimal cardiovascular depression; suppresses adrenal cortisol production; pain on injection; myoclonus; preferred for rapid sequence intubation (RSI) in unstable patients |
| Thiopental (Sodium Pentothal) | Barbiturate | Induction (largely historical); cerebral protection | Ultra-short acting; reduces ICP and cerebral metabolic rate; causes hypotension; precipitates with many drugs; largely replaced by propofol |
| Dexmedetomidine (Precedex) | Alpha-2 agonist | ICU sedation; MAC adjunct; awake craniotomy; fiberoptic intubation | Sedation without respiratory depression; minimal amnesia; analgesic sparing; causes bradycardia and hypotension |
3. Local Anesthetics
Local anesthetics are the drugs most commonly found on the sterile field. They block nerve conduction by inhibiting sodium (Na⁺) channels, preventing depolarization. They are classified as amides or esters based on their chemical structure and metabolism.
3A. Amide vs. Ester Local Anesthetics
| Class | Metabolism | Allergy | Examples |
|---|---|---|---|
| Amides (contain two “i”s in the name) | Liver (hepatic) | Rare; true allergy uncommon | Lidocaine, Bupivacaine, Ropivacaine, Mepivacaine, Prilocaine, Levobupivacaine |
| Esters | Plasma (pseudocholinesterase) | More common; metabolite (PABA) causes allergic reaction | Cocaine, Procaine, Tetracaine, Benzocaine, Chloroprocaine |
Memory Aid: AmIDEs have two “I”s — LIdocaIne, BupIvacaIne, RopIvacaIne
3B. Common Local Anesthetics — Profiles
| Drug | Class | Onset | Duration | Max Dose / Key Notes |
|---|---|---|---|---|
| Lidocaine (Xylocaine) | Amide | Rapid (2–5 min) | 1–2 hrs (plain); 2–4 hrs (with epi) | Plain: 4.5 mg/kg; with epi: 7 mg/kg; also used as antiarrhythmic (IV); most versatile local anesthetic; commonly 1% or 2% on sterile field |
| Bupivacaine (Marcaine, Sensorcaine) | Amide | Slow (5–10 min) | 4–8 hrs (longest duration) | Plain: 2.5 mg/kg; with epi: 3 mg/kg; most cardiotoxic (ventricular fibrillation with overdose); commonly used for spinal anesthesia (0.5% heavy/hyperbaric); post-op wound infiltration; NOT for IV regional |
| Ropivacaine (Naropin) | Amide | Moderate | 3–8 hrs | Similar to bupivacaine but less cardiotoxic; preferred for epidurals (preserves motor function better); used for nerve blocks |
| Mepivacaine (Carbocaine) | Amide | Rapid | 1–3 hrs | Dental/nerve blocks; does not vasodilate like lidocaine; avoid in OB (neonatal toxicity) |
| Cocaine | Ester | Rapid | 30–90 min | Only local anesthetic that is also a vasoconstrictor (inhibits catecholamine reuptake); used topically in ENT (nasal/sinus) surgery; controlled substance (Schedule II); never inject |
| Tetracaine (Pontocaine) | Ester | Moderate | 2–3 hrs | Spinal anesthesia; ophthalmic anesthesia; high potency, high toxicity ester |
| Benzocaine | Ester | Very rapid | Short | Topical only (sprays, gels); risk of methemoglobinemia with excessive use; used before scope insertion |
3C. Epinephrine as a Local Anesthetic Additive
- Purpose: vasoconstriction → reduces systemic absorption → prolongs duration, reduces toxicity, decreases bleeding at injection site
- Concentration typically used: 1:100,000 or 1:200,000 (do NOT use 1:1,000 — 10× more concentrated)
- Contraindicated in “ring” structures: fingers, toes, nose, penis, ear (end-arterial supply → ischemia/necrosis)
- Caution: patients with hypertension, cardiac disease, hyperthyroidism, cocaine use
- On the sterile field: clearly label syringes “with epi” vs. “plain”; never assume
3D. Local Anesthetic Systemic Toxicity (LAST)
LAST occurs when local anesthetic enters the systemic circulation (accidental intravascular injection or excessive dose). It is a medical emergency.
- CNS signs (early): metallic taste, perioral numbness, tinnitus, lightheadedness, agitation → seizures
- Cardiovascular signs (late): arrhythmias, hypotension, cardiac arrest (most severe with bupivacaine)
- Treatment: stop drug, airway support, Intralipid (20% lipid emulsion) — “lipid rescue” traps the anesthetic; avoid vasopressin, beta-blockers, calcium channel blockers during cardiac arrest from LAST
4. Neuromuscular Blocking Agents (NMBAs)
NMBAs cause skeletal muscle paralysis to facilitate intubation and surgical exposure. They work at the neuromuscular junction (NMJ) by blocking acetylcholine receptors. They do NOT cause unconsciousness or analgesia — anesthesia must be maintained separately.
| Drug | Type | Onset / Duration | Key Notes |
|---|---|---|---|
| Succinylcholine (Anectine) | Depolarizing | Onset: 30–60 sec Duration: 5–10 min |
Fastest onset; gold standard for RSI; causes fasciculations; triggers MH; raises serum K⁺ (avoid in burns, crush injuries, denervation); raises IOP and ICP; metabolized by pseudocholinesterase (prolonged in deficiency); NO reversal agent |
| Rocuronium (Zemuron) | Non-depolarizing | Onset: 60–90 sec (high dose: 60 sec) Duration: 30–60 min |
Alternative to succinylcholine for RSI (at high dose); reversed by sugammadex; no histamine release; does NOT trigger MH |
| Vecuronium (Norcuron) | Non-depolarizing | Onset: 2–3 min Duration: 25–40 min |
Intermediate duration; minimal cardiovascular effects; reversed by neostigmine + glycopyrrolate or sugammadex |
| Cisatracurium (Nimbex) | Non-depolarizing | Onset: 2–3 min Duration: 40–60 min |
Metabolized by Hofmann elimination (organ-independent); safe in liver/kidney failure; preferred for ICU patients; no histamine release |
| Atracurium (Tracrium) | Non-depolarizing | Onset: 2–3 min Duration: 20–35 min |
Hofmann elimination; releases histamine (avoid in asthma/allergic patients) |
| Pancuronium (Pavulon) | Non-depolarizing | Onset: 3–5 min Duration: 60–90 min (long) |
Long-acting; causes tachycardia and hypertension (vagolytic); used in long OR cases, cardiac surgery |
4A. Reversal of Neuromuscular Blockade
| Drug | Mechanism | Reverses | Notes |
|---|---|---|---|
| Neostigmine (Prostigmin) | Acetylcholinesterase inhibitor → increases ACh at NMJ | Non-depolarizing NMBAs only | Must give with anticholinergic (glycopyrrolate or atropine) to counteract muscarinic side effects (bradycardia, bronchospasm, increased secretions) |
| Sugammadex (Bridion) | Encapsulates (binds) rocuronium/vecuronium molecules | Rocuronium, Vecuronium | Fast, complete reversal regardless of depth of block; does NOT require anticholinergic co-administration; can reverse even deep block; no muscarinic side effects; increasingly preferred over neostigmine |
5. Opioids & Analgesics
5A. Opioid Analgesics
Opioids are the primary intraoperative analgesics. They act on mu (µ), kappa (κ), and delta (δ) receptors in the CNS and periphery. All cause dose-dependent respiratory depression — the most dangerous adverse effect.
| Drug | Onset / Duration | Key Notes |
|---|---|---|
| Fentanyl (Sublimaze) | IV onset: 1–2 min; duration: 30–60 min | Most common intraoperative opioid; 100× more potent than morphine; no histamine release; risk of “wooden chest syndrome” (chest wall rigidity) with rapid high-dose injection; short duration useful for ambulatory cases |
| Sufentanil | Rapid; duration: 20–45 min | 500–1000× more potent than morphine; used for cardiac surgery, neuroanesthesia, epidurals |
| Remifentanil (Ultiva) | Rapid; duration: 3–10 min (context-sensitive) | Ultra-short acting; metabolized by plasma/tissue esterases (organ-independent); always given as infusion; profound analgesia during case, minimal post-op analgesia; plan post-op pain management |
| Morphine | IV onset: 5–10 min; duration: 3–4 hrs | Gold standard opioid; releases histamine (caution in asthma/allergy); active metabolite accumulates in renal failure; good for post-op pain management; intrathecal morphine provides long-lasting post-op analgesia |
| Hydromorphone (Dilaudid) | IV onset: 5 min; duration: 3–4 hrs | 5–7× more potent than morphine; less histamine release; preferred in renal failure over morphine; used for post-op PCA |
| Meperidine (Demerol) | IV onset: 5 min; duration: 2–4 hrs | Metabolite (normeperidine) causes seizures in renal failure; unique use: treats postoperative shivering; serotonin syndrome risk with MAOIs; falling out of favor |
| Nalbuphine (Nubain) | IV onset: 2–3 min; duration: 3–6 hrs | Mixed agonist-antagonist (kappa agonist, mu antagonist); ceiling effect for respiratory depression; can precipitate withdrawal in opioid-dependent patients; used for pruritus from spinal opioids |
5B. Opioid Reversal
Naloxone (Narcan) — pure opioid antagonist (mu receptor); reverses respiratory depression, sedation, and analgesia; IV onset 1–2 min; duration 30–60 min (shorter than most opioids — re-narcotization risk); administer titrated doses to reverse respiratory depression without reversing analgesia; may precipitate acute withdrawal and severe pain.
5C. Non-Opioid Analgesics
| Drug | Class | Route | Key Notes |
|---|---|---|---|
| Ketorolac (Toradol) | NSAID (COX inhibitor) | IV / IM | Most common IV NSAID in the OR; analgesic + anti-inflammatory; NO opioid side effects; avoid in renal failure, bleeding risk (platelet inhibition), peptic ulcers; max 5 days use; good opioid-sparing agent |
| Acetaminophen (Ofirmev) | Non-opioid analgesic/antipyretic | IV / PO / PR | IV formulation (Ofirmev) used perioperatively; no platelet effect; opioid-sparing; hepatotoxic in overdose or with alcohol; max 4 g/day (1.5 g/day in hepatic disease) |
| Celecoxib (Celebrex) | COX-2 selective NSAID | PO | Reduced GI and platelet side effects vs. non-selective NSAIDs; preoperative “pre-emptive analgesia” protocol; avoid in sulfonamide allergy |
| Gabapentin / Pregabalin | Anticonvulsant / Adjuvant analgesic | PO | Preoperative use reduces opioid requirements; used in multimodal analgesia; treats neuropathic pain; sedation and dizziness are common side effects |
6. Sedatives, Anxiolytics & Hypnotics
| Drug | Class | Key Notes |
|---|---|---|
| Midazolam (Versed) | Benzodiazepine | Most common preoperative anxiolytic/sedative; amnesia, anxiolysis, anticonvulsant, no analgesia; synergistic respiratory depression with opioids; reversed by flumazenil; 0.02–0.05 mg/kg IV |
| Diazepam (Valium) | Benzodiazepine | Longer acting than midazolam; used for muscle spasm, status epilepticus, preoperative anxiety; active metabolites; pain on IV injection (contains propylene glycol) |
| Lorazepam (Ativan) | Benzodiazepine | Longer duration; potent amnesic; ICU sedation; antiemetic; anticonvulsant; no active metabolites (safer in elderly/liver disease) |
| Flumazenil (Romazicon) | Benzodiazepine antagonist | Reverses benzo sedation; shorter half-life than most benzodiazepines — re-sedation risk; can precipitate seizures in benzo-dependent patients |
| Droperidol (Inapsine) | Butyrophenone (antipsychotic) | Antiemetic (low dose); sedative; antipsychotic; QT prolongation (black box warning); used in TIVA for anxiolysis/antiemesis |
| Scopolamine (Transderm Scop) | Anticholinergic | Transdermal patch; preoperative antiemetic; antisialagogue (dries secretions); causes sedation, dry mouth, blurred vision, urinary retention; apply behind ear 4 hrs before surgery |
7. Hemostatic Agents
Hemostatic agents control surgical bleeding. The scrub technologist must know each agent, its preparation, and how it is applied. These are high-yield for the CST exam.
7A. Absorbable Hemostats
| Agent | Composition | How Used | Key Notes |
|---|---|---|---|
| Gelfoam (Gelatin Sponge) | Purified pork skin gelatin | Dry or soaked in thrombin or saline; placed on bleeding surface | Absorbed in 4–6 weeks; provides scaffold for clot formation; may be soaked in thrombin (Gelfoam + thrombin = very effective); count as sponge if large piece used |
| Surgicel (Oxidized Regenerated Cellulose) | Oxidized cellulose fabric/gauze | Applied dry; wrap or pack around bleeding area | Bactericidal properties (low pH); absorbed in 7–14 days; do NOT wet with saline (inactivates it); do NOT use with thrombin; does NOT work in heparinized patients; dark brown color after use (normal) |
| Avitene (Microfibrillar Collagen) | Purified bovine collagen | Applied dry to bleeding surface with dry gloves/instruments | Attracts platelets and activates coagulation cascade; use only dry instruments — moisture causes clumping on gloves; do not use in infected or contaminated wounds; bovine allergy consideration |
| Bone Wax | Beeswax (non-absorbable) | Pressed into bone edges (sternal, skull, long bones) | Mechanical tamponade; not absorbed; impairs bone healing; inhibits osteogenesis; use minimally; not appropriate for infected fields |
7B. Chemical/Biological Hemostats
| Agent | Source / Type | Preparation & Use | Key Notes |
|---|---|---|---|
| Thrombin (Thrombogen, Thrombi-Gel) | Bovine or recombinant human thrombin | Reconstituted with saline; applied topically as liquid or soaked into Gelfoam; NEVER inject IV — fatal | Converts fibrinogen → fibrin directly (bypasses coagulation cascade); available in bovine (may cause antibody formation) or human recombinant forms; must be labeled and passed carefully; topical use ONLY |
| Fibrin Sealant (Tisseel, Evicel) | Human plasma-derived fibrinogen + thrombin | Two-component system mixed at time of application; applied via spray or drops | Mimics final step of coagulation cascade; excellent for parenchymal bleeding (liver, spleen), vascular anastomoses; refrigerated storage; thaw before use; human-derived (blood product considerations) |
| Epinephrine (topical) | Catecholamine / vasoconstrictor | Diluted to 1:100,000 or 1:200,000; soaked into pledgets/sponges; applied to mucosal surfaces | Powerful vasoconstriction reduces blood loss; common in ENT, plastic, ophthalmology; systemic absorption can cause tachycardia/hypertension; label clearly on sterile field |
| Silver Nitrate | Chemical cauterizing agent | Applicator sticks (75% silver nitrate); applied to skin or mucous membrane bleeding points | Chemical cautery; turns tissue black; used for umbilical granulomas, nosebleeds, minor skin bleeding; protect surrounding tissue |
| Tranexamic Acid (TXA) | Antifibrinolytic | IV infusion or topical irrigation | Inhibits fibrinolysis (prevents clot breakdown); reduces blood loss in major surgeries (trauma, cardiac, orthopedic, OB); does NOT form clots directly; must administer within 3 hrs of injury for trauma |
8. Anticoagulants, Antiplatelets & Reversal Agents
| Drug | Mechanism | OR Relevance | Reversal |
|---|---|---|---|
| Heparin (unfractionated) | Activates antithrombin III → inhibits thrombin and Factor Xa | Vascular surgery, cardiac bypass (systemic heparinization); heparin-soaked irrigation; DVT prophylaxis (SQ); flush for lines | Protamine sulfate (1 mg per 100 units heparin); can cause hypotension, anaphylaxis in fish/vasectomy patients |
| Enoxaparin (Lovenox) | Low-molecular-weight heparin (LMWH); inhibits Factor Xa > thrombin | DVT/PE prophylaxis and treatment; hold before elective surgery (12–24 hrs) | Protamine sulfate (partial reversal only; ~60% effective); not monitored by PTT |
| Warfarin (Coumadin) | Inhibits Vitamin K-dependent clotting factors (II, VII, IX, X) | Held 5 days before elective surgery; monitor INR; bridging therapy with heparin if high thromboembolic risk | Vitamin K (slow reversal, 6–24 hrs) or Fresh Frozen Plasma (FFP) (immediate); 4-factor PCC for emergency reversal |
| Dabigatran (Pradaxa) | Direct thrombin inhibitor (DOAC) | Hold 24–48 hrs before elective surgery; no routine lab monitoring | Idarucizumab (Praxbind) — specific reversal agent |
| Rivaroxaban (Xarelto), Apixaban (Eliquis) | Direct Factor Xa inhibitors (DOACs) | Hold 24–48 hrs before elective surgery | Andexanet alfa (Andexxa) — specific reversal; 4-factor PCC as alternative |
| Aspirin | Irreversible COX-1 inhibitor → inhibits TXA₂ → platelet aggregation inhibition | Typically held 7–10 days before elective surgery (platelet lifespan); continued for cardiac stents | No reversal agent; platelet transfusion if emergent |
| Clopidogrel (Plavix) | ADP receptor blocker → platelet aggregation inhibition | Hold 5–7 days before elective surgery; continued for coronary stents (critical — stopping can cause stent thrombosis) | No reversal; platelet transfusion if bleeding |
9. Cardiovascular Drugs in the OR
| Drug | Class / Action | OR Use |
|---|---|---|
| Epinephrine (Adrenalin) | Alpha + Beta agonist; vasopressor, cardiac stimulant, bronchodilator | Cardiac arrest (1 mg IV q 3–5 min); anaphylaxis (0.3–0.5 mg IM); local anesthetic additive; topical vasoconstriction |
| Atropine | Anticholinergic (muscarinic antagonist) | Bradycardia (0.5–1 mg IV); antisialagogue (dries secretions); reverses cholinergic effects of neostigmine; given with neostigmine for NMBA reversal |
| Glycopyrrolate (Robinul) | Anticholinergic; does NOT cross blood-brain barrier | Given with neostigmine (preferred over atropine — smoother HR response); antisialagogue; reduces GI secretions |
| Ephedrine | Indirect sympathomimetic (releases catecholamines) | Hypotension treatment (especially spinal/epidural hypotension); increases HR and BP; safe in obstetrics; 5–25 mg IV bolus |
| Phenylephrine (Neo-Synephrine) | Pure alpha-1 agonist; vasopressor | Hypotension without tachycardia; preferred in cardiac disease; causes reflex bradycardia; common infusion in OR; also topical nasal decongestant |
| Vasopressin (ADH) | V1 receptor agonist; potent vasoconstrictor | Cardiac arrest (vasopressor); septic shock; GI vasoconstriction (esophageal varices surgery); topical in GYN (reduces blood loss) |
| Labetalol | Alpha + Beta blocker; antihypertensive | Intraoperative hypertension; controlled hypotension techniques; safe in pregnancy (OB emergencies) |
| Nitroglycerin | Nitrate vasodilator; primarily venodilator | Hypertensive urgency; cardiac ischemia; controlled hypotension; IV or sublingual; headache is common side effect |
| Sodium Nitroprusside (Nipride) | Arterial + venous vasodilator | Controlled hypotension (neurosurgery, aortic surgery); immediate onset/offset; cyanide toxicity with prolonged use; protect from light (light-sensitive); monitor thiocyanate levels |
| Adenosine | Slows AV node conduction | SVT termination; 6 mg rapid IV push followed by saline flush; very short half-life (10 sec); transient asystole (warn patient/team); must be given into central or large antecubital vein |
10. Antibiotics & Prophylaxis in the OR
Surgical antibiotic prophylaxis (SAP) is one of the most important SSI prevention measures. Key principles:
- Timing: Administer within 60 minutes before incision (vancomycin and fluoroquinolones within 120 minutes due to longer infusion time)
- Redosing: Repeat dose if case exceeds two half-lives of the antibiotic or if significant blood loss (>1,500 mL)
- Duration: Discontinue within 24 hours post-incision (48 hrs for cardiac surgery); prolonged prophylaxis does NOT reduce SSI and promotes resistance
- First-line agent: Cefazolin (Ancef) — first-generation cephalosporin; covers most skin flora (G+ cocci, some G−); used for most clean and clean-contaminated cases
| Procedure Type | Preferred Agent(s) | PCN Allergy Alternative |
|---|---|---|
| Most clean/clean-contaminated surgeries | Cefazolin | Clindamycin or Vancomycin |
| Colorectal surgery | Cefazolin + Metronidazole (or Cefoxitin alone) | Clindamycin + Gentamicin or Aztreonam |
| Cardiac / vascular (prosthetic) | Cefazolin (Vancomycin added if MRSA risk) | Vancomycin |
| Neurosurgery | Cefazolin | Clindamycin or Vancomycin |
| GU surgery | Cefazolin or Fluoroquinolone | Gentamicin ± Vancomycin |
| OB/GYN (Cesarean section) | Cefazolin (before incision, not cord clamp) | Clindamycin + Gentamicin |
Antibiotic Wound Irrigation
Antibiotic irrigation is used to reduce bacterial contamination in the wound before closure. Common preparations on the sterile field include:
- Bacitracin irrigation — 50,000 units in 500 mL saline; used in orthopedic, cardiac, and neurosurgical cases; avoid in renal failure (nephrotoxic if absorbed)
- Gentamicin irrigation — G− coverage; common in joint surgery
- Vancomycin powder — applied directly to wound before closure (especially spinal surgery); reduces SSI; systemic absorption is minimal
- Neomycin-Polymyxin B (Neosporin) — topical only; broad-spectrum coverage on skin wounds
11. Diuretics, IV Fluids & Electrolyte Agents
11A. Diuretics
| Drug | Class | OR / Surgical Use |
|---|---|---|
| Furosemide (Lasix) | Loop diuretic | Reduce cerebral edema (ICP), pulmonary edema; used intraoperatively when fluid overloaded; rapid IV onset; monitor K⁺ (hypokalemia) |
| Mannitol | Osmotic diuretic | Reduce ICP and IOP (neurosurgery, ophthalmology, trauma); increases urine output; given IV over 20–30 min; use in-line filter (may crystallize); avoid in anuric patients |
| Acetazolamide (Diamox) | Carbonic anhydrase inhibitor | Reduce IOP (glaucoma surgery, ophthalmology); decrease CSF production; mild diuresis |
11B. IV Fluids Used in the OR
| Fluid | Type | Use / Notes |
|---|---|---|
| Normal Saline (0.9% NaCl) | Isotonic crystalloid | Most versatile; compatible with blood products and most drugs; large volumes cause hyperchloremic metabolic acidosis; used for irrigation (wounds, urological) |
| Lactated Ringer’s (LR) | Isotonic balanced crystalloid | Most physiologically similar to plasma; preferred for large-volume resuscitation; DO NOT infuse with blood products (calcium causes clotting); slightly hypotonic |
| D5W (5% Dextrose in Water) | Hypotonic once metabolized | Drug diluent; maintenance fluid; NOT for resuscitation; can cause cerebral edema with large volumes; avoid in hyperglycemia |
| Albumin (5% or 25%) | Colloid | Volume expansion; hypoalbuminemic patients; stays in vascular compartment longer than crystalloids; expensive; used in liver surgery, burns, paracentesis |
| Sterile Water for Irrigation | Hypotonic | Urological procedures (cystoscopy, TURP); NOT for IV use — causes hemolysis; used in field to lyse red blood cells during laparoscopic procedures (when bladder tumor removed) |
12. Ophthalmic Drugs
Ophthalmic drugs are commonly found on the sterile field for eye surgeries (cataract, vitreoretinal, corneal, glaucoma). These are frequently tested on the CST exam.
| Drug | Action | Use | Notes |
|---|---|---|---|
| Balanced Salt Solution (BSS) | Irrigation / viscoelastic maintenance | Intraocular irrigation during cataract, vitreoretinal surgery | Isotonic; ph and electrolyte composition similar to aqueous humor; does not harm endothelium |
| Viscoelastics (OVDs) (Healon, Provisc, Viscoat) |
Protect corneal endothelium; maintain space | Cataract surgery (maintain anterior chamber); lens implant placement | Hyaluronic acid or chondroitin sulfate; must be removed at end of case (elevates IOP if left in) |
| Miochol (Acetylcholine) | Miotic — constricts pupil | Intraocular; rapid pupil constriction after lens implant in cataract surgery | Reconstituted immediately before use (short stability); intraocular injection only; very short acting |
| Miostat (Carbachol) | Miotic (more potent and longer-acting than acetylcholine) | Intraocular miosis; glaucoma | Longer duration than acetylcholine; intraocular use; systemic absorption can cause bradycardia, sweating |
| Phenylephrine (ophthalmic) | Mydriatic (dilates pupil); alpha-1 agonist | Preoperative pupil dilation for cataract surgery | 2.5% or 10% drops; systemic absorption of 10% can cause hypertension |
| Atropine (ophthalmic) | Mydriatic and cycloplegic (paralyzes accommodation) | Pupil dilation; amblyopia treatment; anterior uveitis | Long-acting (days); systemic absorption (especially in children) causes anticholinergic effects; press lacrimal duct after instillation to reduce absorption |
| Timolol (ophthalmic) | Beta-blocker; reduces aqueous humor production | Glaucoma (reduce IOP) | Systemic absorption can cause bradycardia, bronchospasm (avoid in asthma/COPD) |
| Fluorescein | Diagnostic dye | Corneal staining to detect abrasions, ulcers; retinal angiography (IV) | Turns tears/urine orange-yellow; IV form used in fluorescein angiography |
13. Antiemetics
Postoperative nausea and vomiting (PONV) is one of the most common surgical complications. Risk factors include female sex, history of PONV or motion sickness, non-smoking status, use of opioids/volatile anesthetics, and longer surgical duration.
| Drug | Class / Mechanism | Key Notes |
|---|---|---|
| Ondansetron (Zofran) | 5-HT₃ receptor antagonist | Most common antiemetic in OR; given at end of case; minimal side effects; QT prolongation in high doses; headache common |
| Dexamethasone (Decadron) | Corticosteroid; antiemetic mechanism not fully understood | Given at induction; prevents PONV; also reduces laryngeal edema, airway swelling; anti-inflammatory; caution in diabetics (hyperglycemia); 4–8 mg IV |
| Metoclopramide (Reglan) | Dopamine (D2) antagonist; prokinetic | Antiemetic + gastric motility agent; increases LES tone (aspiration prophylaxis); EPS (extrapyramidal) side effects (dystonia) with high doses; 10 mg IV |
| Promethazine (Phenergan) | Antihistamine (H1 blocker) + anticholinergic | Antiemetic, sedative; causes significant sedation; IV injection risk — can cause tissue necrosis if extravasation (black box warning against IV push); preferred IM or deep IV diluted |
| Scopolamine (patch) | Anticholinergic | Applied behind ear at least 4 hrs before surgery; effective for motion sickness / PONV in high-risk patients; causes dry mouth, blurred vision, urinary retention, confusion (especially elderly) |
14. Malignant Hyperthermia (MH) — Critical Emergency
⚡ Malignant Hyperthermia is a life-threatening pharmacogenetic emergency — one of the highest-yield topics on the CST exam.
Definition: A hypermetabolic crisis of skeletal muscle triggered by specific anesthetic agents in genetically susceptible individuals. Caused by a defect in the ryanodine receptor (RYR1 gene mutation) → uncontrolled Ca²⁺ release from sarcoplasmic reticulum → sustained muscle contraction and heat production.
Triggering Agents:
- All halogenated volatile anesthetics: sevoflurane, desflurane, isoflurane, halothane, enflurane
- Succinylcholine (depolarizing NMBA)
Signs & Symptoms (earliest to latest):
- Earliest sign: Unexplained rise in end-tidal CO₂ (EtCO₂) — cannot be corrected by increasing ventilation
- Masseter muscle rigidity (especially after succinylcholine) — jaw locked closed
- Generalized muscle rigidity
- Tachycardia, arrhythmias
- Hyperthermia — temperature may rise >1°C every 5 min; late sign but most dramatic
- Sweating, mottled skin, cyanosis
- Metabolic acidosis, hyperkalemia, myoglobinuria (cola-colored urine) → renal failure
Treatment (MHAUS Protocol):
- Call for help; activate MH protocol; have someone call MHAUS hotline: 1-800-MH-HYPER
- Discontinue all triggering agents immediately — stop volatile anesthetic and succinylcholine
- Switch to non-triggering anesthetic (propofol TIVA)
- Hyperventilate with 100% O₂ at high flows (>10 L/min)
- Administer Dantrolene sodium (Dantrium) — 2.5 mg/kg IV bolus; repeat every 5 min until symptoms resolve; max ~10 mg/kg; mix with sterile water (NOT saline — precipitates); very difficult to reconstitute quickly
- Active cooling: ice packs to groin/axilla, cold IV saline, cold gastric lavage; stop when temp <38°C (avoid overshoot hypothermia)
- Treat hyperkalemia (calcium chloride, sodium bicarbonate, insulin/dextrose, Kayexalate)
- Treat arrhythmias (amiodarone, avoid calcium channel blockers — interact with dantrolene)
- Maintain urine output >2 mL/kg/hr (prevents myoglobin-induced renal failure) — Foley catheter, IV fluids, furosemide or mannitol
- Continue dantrolene for 24–48 hrs post-episode to prevent recurrence
- Transfer to ICU
MH Cart must contain: Dantrolene (36 vials minimum), sterile water for reconstitution, syringes, sodium bicarbonate, calcium chloride, insulin/dextrose, cooling supplies, lab specimen tubes.
15. Anaphylaxis in the OR
Anaphylaxis is a severe, life-threatening allergic reaction. Under anesthesia, the presentation is often atypical — urticaria/flushing may be hidden by drapes.
Common Triggers in the OR
- Neuromuscular blocking agents (most common cause — especially rocuronium, succinylcholine)
- Latex — Type I (IgE-mediated) or Type IV (delayed); high-risk: spina bifida patients, healthcare workers with prolonged exposure, individuals with multiple surgeries or banana/avocado/kiwi allergy (“latex-fruit syndrome”)
- Antibiotics — beta-lactams (especially penicillin); cephalosporins (cross-reactivity ~1–2%)
- IV contrast media
- Chlorhexidine — increasingly recognized cause of intraoperative anaphylaxis
- Blood products, protamine, vancomycin
Signs of Anaphylaxis Under Anesthesia
- Cardiovascular: hypotension, tachycardia (most common presentations under anesthesia)
- Respiratory: bronchospasm, increased peak airway pressure, hypoxia
- Skin: erythema, urticaria, angioedema (may be hidden by drapes)
Treatment of Anaphylaxis
- Stop suspected trigger(s)
- Epinephrine 0.3–0.5 mg IM (vastus lateralis) or IV for cardiac arrest; first-line and definitive treatment
- 100% O₂; secure airway
- IV fluid bolus (1–2 L normal saline) for hypotension
- Diphenhydramine (Benadryl) — H1 blocker; 25–50 mg IV
- Ranitidine or famotidine — H2 blocker (add to antihistamine coverage)
- Methylprednisolone or hydrocortisone — steroids; reduce late-phase reaction; not helpful for acute episode
- Bronchospasm: albuterol nebulization, IV epinephrine, magnesium sulfate
Latex Allergy — OR Management
- Latex-safe OR: all latex products removed (gloves, tubing, Foley, tourniquets, stoppers, etc.)
- Schedule latex-allergic patients as first case of the day — lowest latex aeroallergen levels
- Use latex-free gloves, non-latex Foley catheters, latex-free IV tubing and bags
- Premedicate if prescribed: diphenhydramine + corticosteroid the night before and morning of surgery
- Have epinephrine drawn and immediately available
16. Irrigating Solutions & Other Field Agents
| Solution / Agent | Use | Key Notes |
|---|---|---|
| Normal Saline (0.9%) | General wound irrigation; sponge/instrument moistening | Universal irrigant; compatible with all tissues; used to keep the field moist and irrigate cavities |
| Lactated Ringer’s | Abdominal/thoracic irrigation; peritoneal lavage | More physiologic; preferred for large-volume peritoneal irrigation |
| Sterile Water | Urological (cystoscopy, TURP); bladder irrigation | NEVER IV; causes hemolysis; used in bladder procedures where visualization requires clear fluid; used to lyse RBCs when tumor cells must not implant |
| Glycine 1.5% | TURP distending/irrigating medium | Non-electrolyte (safe with electrosurgery); large volumes absorbed can cause TURP syndrome (hyponatremia, fluid overload, encephalopathy — vision changes, confusion) |
| Sorbitol / Mannitol | Hysteroscopy distending media; urological | Non-electrolyte; risk of fluid absorption in hysteroscopy (fluid deficit monitoring required); mannitol provides diuretic effect to offset absorption |
| Hyskon (Dextran 70) | Hysteroscopy distending medium | Viscous; very effective at distension; risk of anaphylaxis; risk of DIC with excessive absorption; difficult to clean instruments (must clean immediately) |
| Methylene Blue | Diagnostic dye; tissue marking | Identify ureters during pelvic surgery; sentinel lymph node mapping; fistula identification; turns urine blue; treat methemoglobinemia; serotonin syndrome risk with serotonergic drugs |
| Isosulfan Blue / Patent Blue | Sentinel lymph node mapping | Injected around tumor; localizes sentinel lymph node(s) for biopsy; anaphylaxis risk (2%); stains tissue blue; urine turns blue-green |
| Indigo Carmine | Ureteral visualization / bladder integrity | IV injection; turns urine blue-green — confirms ureteral patency intraoperatively; used during pelvic surgery, hysterectomy, ureteral repair |
17. Controlled Substances & DEA Schedules
Controlled substances in the OR are regulated by the DEA (Drug Enforcement Administration). The scrub technologist must understand that any drug wasted or discarded must be witnessed and documented. Common OR controlled substances:
| Schedule | Criteria | OR Examples |
|---|---|---|
| Schedule I | High abuse potential; no accepted medical use | Heroin, LSD, psilocybin (not used in OR) |
| Schedule II | High abuse potential; severe dependence; accepted medical use | Fentanyl, morphine, hydromorphone, oxycodone, cocaine, methamphetamine, methadone |
| Schedule III | Moderate abuse potential; accepted medical use | Ketamine, anabolic steroids, buprenorphine, codeine combinations |
| Schedule IV | Low abuse potential; accepted medical use | Midazolam, diazepam, lorazepam, tramadol, zolpidem |
| Schedule V | Lowest abuse potential | Cough syrups with codeine, pregabalin |
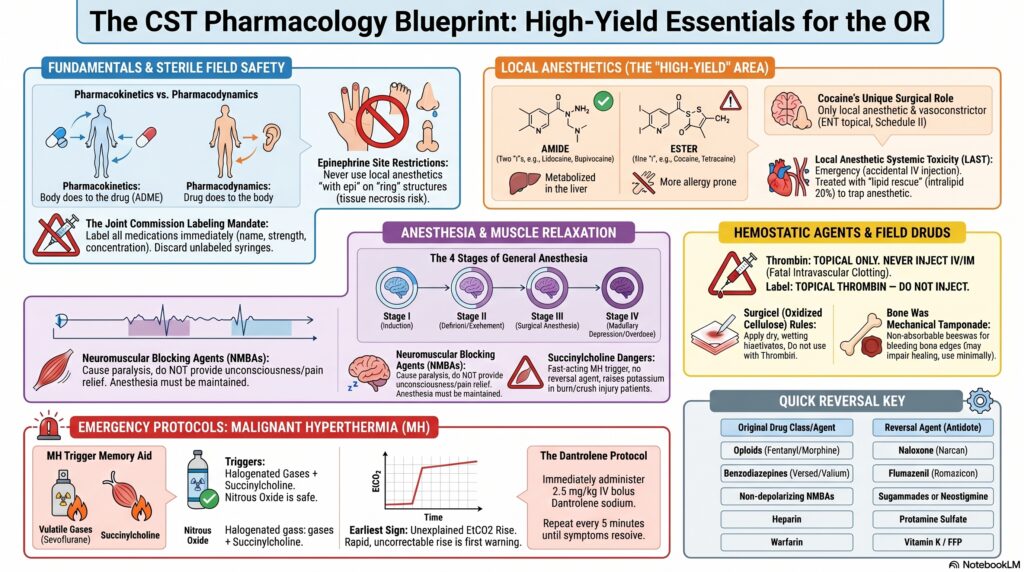
⚡ High-Yield Exam Quick Reference
Label ALL Field Drugs
Every medication on the sterile field must be labeled immediately with drug name, concentration, and relevant info. Unlabeled syringes = discard. TJC mandate.
MH Triggers vs. Safe Drugs
Triggers: All halogenated volatiles + succinylcholine
Safe: Propofol, ketamine, etomidate, N₂O, opioids, benzodiazepines, non-depolarizing NMBAs
Treatment: Dantrolene 2.5 mg/kg IV
Amide vs. Ester LAs
Amides (two “i”s): Lidocaine, Bupivacaine, Ropivacaine → liver metabolism
Esters: Cocaine, Tetracaine, Benzocaine, Procaine → plasma esterases; PABA allergy
Epinephrine Sites — NEVER Use
Never inject epi “with local” into: fingers, toes, nose, ears, penis (ring/end-arterial structures) → ischemia and necrosis.
Thrombin — TOPICAL ONLY
NEVER inject thrombin IV or IM — causes fatal intravascular clotting. Always label: “TOPICAL THROMBIN — DO NOT INJECT.”
Surgicel — Use DRY Only
Surgicel (oxidized cellulose) must be applied dry. Do NOT wet with saline — inactivates it. Do NOT combine with thrombin.
Reversal Agents — Must Know
Opioids → Naloxone (Narcan)
Benzodiazepines → Flumazenil
Non-depol NMBAs → Neostigmine (+ glycopyrrolate) or Sugammadex
Heparin → Protamine sulfate
Warfarin → Vitamin K / FFP
Cocaine — Unique Properties
Only local anesthetic that is also a vasoconstrictor. Topical use only (ENT). Schedule II controlled substance. Never inject.
Succinylcholine — Special Dangers
Triggers MH. Raises K⁺ (avoid in burns, crush injury, paralysis). Raises IOP and ICP. Has NO reversal agent. Fastest-onset NMBA (RSI gold standard).
Antibiotic Prophylaxis Timing
Cefazolin within 60 min before incision. Vancomycin/fluoroquinolones within 120 min. Redose q 4 hrs (cefazolin) or with major blood loss. Stop within 24 hrs post-op.
Ophthalmic Miotics vs. Mydriatics
Miotics (constrict pupil): Miochol (acetylcholine), Miostat (carbachol), Pilocarpine
Mydriatics (dilate pupil): Phenylephrine, Atropine, Tropicamide
TURP Syndrome
Caused by absorption of glycine 1.5% irrigant during TURP. Results in dilutional hyponatremia → visual changes, confusion, bradycardia. Treat with hypertonic saline (3% NaCl) and furosemide.
© 2026 Coy Academy. All rights reserved. No part of this material may be reproduced or transmitted in any form or by any means without the prior written permission of Coy Academy.